Red Light Therapy has been utilized in human clinical trials to support spot fat reduction, body contouring, and weight management. As such, Red Light Therapy holds great potential to be used for the obesity epidemic.
However, marketing of these weight loss claims is often so heavy-handed that the consumer must assume spontaneous fat loss is a common side effect of Red Light Therapy.
Red Light Therapy is often utilized on the face for anti-aging benefits, wrinkle reduction, acne management, and overall complexion benefits. [1][2]
However, there are now concerns that it may result in unwanted facial fat loss.
As always, Red Light Therapy presents a double-edged sword. The biphasic nature and complexity of the treatment offers a wide range of contradicting effects.
Executive Summary:
Does Red Light Therapy Cause Facial Fat Loss?
- Facial fat loss is a product of natural aging, rapid weight loss, excessive sunlight exposure (photoaging), malnutrition, and some diseases and medications.
- Red Light Therapy may be falsely correlated with facial fat loss as it is often implemented in the age ranges (20-40's) that natural facial fat loss is already occurring.
- Red Light Therapy can reduce fluid retention and inflammation of the face, theoretically resulting in the appearance of reduced facial volume.
- Properly designed Red Light Therapy treatments have been shown to improve facial volume by supporting the proliferation of facial structures.
- Excessive Red/NIR intensities and/or heat are to be avoided for facial treatments, typically less than 35mW/cm^2 is recommended for skincare.
- Facial fat and abdominal fat are metabolically and functionally different, so the parameters that aid abdominal fat loss would likely not work the same on facial fat.
Body Weight and Body Fat:
- Sunlight, Sleep, Melatonin, and Vitamin D are vital for managing obesity and reducing weight. All of which are related to proper and/or therapeutic light exposure.
- Red Light Therapy alone does not consistently produce weight loss effects.
- Body Contouring (spot fat reduction) is possible with Red Light Therapy but it's mechanisms and parameters are still not fully understood.
- Exercise is strongly recommended to be used in conjunction with Red Light Therapy particularly for the goals of weight loss and body contouring.
- Weight gain is possible from Red Light Therapy when combined with poor diet, no exercise, and improper parameters.
- Weight loss from Red Light Therapy is not consistently statistically significant, and typically only results in an average loss of 1-3 kg (2.2-6.6lbs). Which is regarded as being not clinically meaningful as an intervention for obesity.
- Red Light Therapy can support weight management in indirect ways like promoting muscle growth, reduced muscle soreness from workouts, improved sleep, reduced inflammation, and improved blood sugar and insulin regulation.
Facial Fat Loss and Taxes:
Aging is an important factor for facial fat loss. Infants generally have rounded features and higher facial fat (i.e. the "baby face" is one of having chubby cheeks). A sign of maturity is indeed a more slim face than our youth.
As the quotes below describe, as we age we generally experience atrophy (loss) of the deep fat tissue.
"With the increase of age, the change of fat interval position leads to the change of adipose tissue contour [13]. Generally, these changes include atrophy of the deep fat tissue and displacement and hypertrophy of the shallow fat tissue [11, 13]." [3]
And:
"Facial lipoatrophy refers to the loss of subcutaneous fat tissue presenting by flattening or indentation of convex contour of the face. Facial lipoatrophy is a feature of the normal ageing process." [4]
And:
"intrinsic aging is known in general to correlate with a continuous reduction of subcutaneous white adipose tissue (sWAT) and concur-rent accumulation of visceral fat [10]" [5]
Gradual facial volume reduction starts around age 20, with more significant changes in the 30's.
"A significant decrease in fat volume in cheeks, temples and orbits starts to be visible at the age of 20, however changes in contour of the face begin to be noticeable roughly at the age of 30 [4]." [4]
Another article describes in great detail what people should expect from the facial aging process, where in the 40's they note:
"Midface loses projection, hollows, and appears to descend39" [6]
This may explain a strong correlation of usage of Red Light Therapy and facial fat loss. Since Red Light Therapy is most often implemented during the age ranges where facial fat loss from natural aging is already becoming apparent. This can lead to false accusations that the Red Light Therapy is the root cause, when it may have been naturally occurring already.
The goal of anti-aging is not necessarily to stop or reverse aging, but to embrace the aging process gracefully.
"Aging gracefully may be synonymous with retaining fullness of features, smooth facial contours, gradual transitions between facial areas, and proper proportions in 3 dimensions while showing only a modicum of lines, blemishes, hollows, and shadows." [6]
Indeed, adults with heavier faces are generally correlated with being less healthy.
"Studies also consistently report that people with lower perceived facial adiposity are rated as more attractive and healthier compared to people with higher perceived facial adiposity (Klaczynski et al., 2009; Rantala et al., 2013a; Han et al., 2016; Foo et al., 2017). " [7]
A balance must be struck to maintain a mature face but that is not too heavy on one end and not too gaunt on the other end.
Ozempic Face and Facial Fat Loss:
The factors for accelerated facial aging primarily include:
- Photoaging (Excessive Ultraviolet, Blue, Sunlight, Infrared Heating, etc)
- Malnutrition [8]
- Specific diseases
- Specific medications and drugs
"diet or illness affects facial volumes in particular; the continuing effect of gravity pulls skin down; our behavior regarding ultraviolet (UV) exposure degrades skin quality; and finally, our lifestyle choices, such as smoking, may be responsible for premature aging by generating noxious free radicals. Facial aging is the result of several concomitant processes." [9]
A popular class of drugs called Glucagon-like peptide-1 (GLP-1) receptor agonists include Ozempic and Weygovy. Both use the same active ingredient called semaglutide.
These drugs have been found to promote weight loss through various mechanisms including reducing appetite, reduced food intake, slowed gastric emptying, and glucose/insulin regulation. [10]
The rapid weight loss obtained from these types of drugs has been associated with loss of facial volume and the appearance of advanced facial aging. This has been dubbed "Ozempic Face". We can examine the aspects of this phenomenon and later relate them to what we know about how Red Light Therapy can improve the face.
A description of Ozempic Face from one article is:
"Accordingly, patients report significant facial fat loss, resulting in an array of cosmetic changes, including the development of wrinkles, sunken eyes, a hollowed appearance, sagging jowls around the neck and jaw, and alterations in the cheeks, lips, and chin." [11]
Presumably this side effect is caused by facial fat pad reduction. There is debate if the Semaglutide is specifically causing unnatural facial fat loss, or if this a normal occurrence from any sort of rapid weight loss.
For example, facial fat loss is also reported as a side effect of bariatric surgery (gastric bypass surgery). Which often results in a 60% reduction in excess body weight in 6 months. [12]
One article notes that rapid weight loss can cause the face to appear 5 years older than the chronological age. Even when the person returns to a healthy weight the changes to the face may remain. [13]
However, Ozempic Face is not just 1) the loss of facial fat. It is also correlated with 2) a loss of facial muscle and 3) reduction of collagen and elastin production.
"The accelerated facial aging and altered skin health observed in GLP-1RA patients appears to be multifactorial, involving loss of dermal and subcutaneous white adipose tissue, and altered proliferation and differentiation of adipose-derived stem cells (ADSCs), and impacts on the production and secretion of hormonal and metabolic factors. These changes compromise the structural integrity and barrier function of the skin and may lead to diminished facial muscle mass, further exacerbating the appearance of aging." [14]
Indeed, the natural loss of facial volume is commonly attributed to many factors, not just the fat. So we must consider how Red Light Therapy affects several of these factors to preserve facial volume.
"Facial aging is an intricate process involving interrelated changes to bone, muscle, fat, and skin." [6]
As is common with rapid weight loss, a proportion of the weight loss is due to fat and some portion is muscle loss. The key is to preserve muscle while losing fat.
Weight loss from Ozempic maybe from up to 40% lean mass (i.e. muscle). Thus, also potentially losing volume and structure of the facial contours in the facial muscles.
"While the lean mass remained stable in some cases, notable reductions ranging from almost 0% to 40% of total weight reduction were observed in others." [15]
The undereating from these drugs also promotes malnutrition and poor collagen maintenance.
"Although this may benefit a patient’s weight management efforts, if patients do not prioritize and consume sufficient protein, they face significant risk of lean mass weight loss. This leads to malnutrition, sarcopenia, and poor wound healing." [13]
Prioritizing protein consumption during a weight loss effort may help preserve facial muscle and collagen production.
Ozempic Face and Red Light Therapy:
Conventional recommendations for treating facial fat loss (i.e. from semaglutide drugs) include dermal fillers and surgery like fat grafts. [14]
Minimally invasive clinical treatments for Ozempic Face include RadioFrequency, Microneedling, and Laser Skin Tightening.
"Radiofrequency, microneedling, and laser skin tightening modalities can revitalize the skin and promote collagen and elastin production." [13]
While not specifically studied for "Ozempic Face", we could easily make a case for using Red Light Therapy during and after usage of a semaglutide treatment to preserve facial health.
1) Preserve facial fat. Contrary to popular belief, there are mechanisms that Red Light Therapy can actually promote and preserve fat cells. [64][71][72]
2) Preserve facial muscle. Studies have shown that PBM improves muscle performance, supports muscle hypertrophy, and prevents muscle atrophy. [16] This is shown not only for athletes but more importantly in aging populations. [17][18][19]
3) Improves Collagen and Elastin Production. Famously, photobiomodulation treatments are utilized for anti-aging, anti-wrinkles, and overall skin health. Often resulting in the appearance of improved facial volume. As we will review in the next sections.
Photobiomodulation Restores Facial Volume
Photobiomodulation is often employed for anti-aging and facial rejuvenation. It promotes the proliferation of connective tissues, collagen, and elastin. Many studies have confirmed it can decrease the volume of wrinkles and increase elasticity. Thus, delivering a fuller, tighter, youthful appearance of the face.
Aging naturally leads to reduced production of connective tissue, less facial muscle, and less facial fat - leading to shallow or sagging facial features. Advanced facial aging from rapid weight loss or malnutrition would also accelerate these problems.
"Aging has a detrimental effect on connective tissue in the skin, leading to declines in elastin and collagen fibers and thus resulting in fine lines and wrinkles [3]." [84]

An April 2024 article titled "Unlocking the Power of Light on the Skin: A Comprehensive Review on Photobiomodulation" makes clear of the anti-aging effects:
"In summary, PBM activates cellular mechanisms such as photothermolysis and wound healing, which generates a new extracellular matrix with components, such as new collagen fibers, elastin, and others, which contribute to the restoration of skin elasticity and a more youthful appearance." [2]
Photobiomodulation is well known to reduce the appearance of wrinkles as noted in the following two articles:
"Clinically, this manifested as reduced wrinkles and improved skin elasticity" [20]
"In addition to reducing wrinkles, it stimulates fibroblasts and thus increases the production of collagen and elastin. 9" [1]
As the following article shows a 30% reduction in wrinkle volume, thus improving the appearance of volume for the face.
"PBM, both at red and amber wavelengths, is an effective tool for rejuvenation, producing a 30% wrinkle volume reduction."[21]
As far as we can find, there are hardly ever side effects reported from these Red Light Therapy studies, notably no complaints of facial fat loss.
Quite the opposite; when asked, the participants will report a positive subjective improvement in youthful appearance.
"The participants perceived the greatest improvement in fine lines and wrinkles, skin texture, and youthful appearance." [22]
From the quote below it appears that clinicians do not appear to believe that LED light therapy has any direct effect on deep facial structures at all.
"The use of LED devices brings practicality and safety to applications and has also been evaluated for facial rejuvenation, mainly in the red wavelength.[17] PBM is indicated for mild facial photoaging, fine wrinkles, skin damage, and texture changes. They are not indicated as replacement therapy for loss of volume, facial contour, sagging skin, or deep rhytids.[25" [23]
One article does note that Near-Infrared is preferred for skincare to treat deeper wrinkles on the face.
"NIR was able to reduce deeper wrinkles but was not as effective in reducing pigment as RL. All clinical trials reported that PBM was a safe, athermal treatment with no side effects. PBM is safe and can be applied as a treatment for wrinkles and photoaging." [2]
While NIR is unjustly demonized for facial skincare, it is likely due to excessive intensity and heating. As the above quote notes that it is "athermal" meaning there is no heat.
Intensity Matters for Skincare
Dr. Daniel Barolet has written several peer-reviewed articles noting that NIR intensity of up to 35 mW/cm^2 will trigger beneficial skincare effects. Higher intensities (specifically citing >100mW/cm^2) will risk photoaging.
"Such a biphasic pattern may explain the reported increase in MMP-1 and ROS/LOS following high IR-A irradiance (i.e., >100 mW/cm2), inducing skin hyperthermia with subsequent heat-related detrimental effects. Conversely, lower irradiance (<50 mW/cm2) does not induce skin hyperthermia as in PBM." [24]
As usual, it is strongly advised to use intensities lower than 50 mW/cm^2, particularly for skincare.
Additionally from the same article, excess heat is also correlated with reduced skin health.
"Actually, a relatively small increase in temperature may induce collagen degradation and reactive oxygen species (ROS) generation." [24]
Since Photobiomodulation is by-definition a non-thermal therapy using light, then a properly designed device and protocol would easily avoid such an issue.
One major mechanism with high intensities and/or heat is the activation of the enzyme MMP-1 in the skin. One study describes it as:
"Matrix metalloproteinase-1 (MMP-1) is a zinc-containing endopeptidase that degrades dermal collagen and other extracellular matrix molecules. " [25]
Thus, when MMP-1 is activated by high intensity NIR light and/or heat, then the resulting loss of collagen would lead to a loss of facial volume.
An article on Photoaging of the skin notes this role of MMPs on the skin. Most notably MMPs are activated from UV exposure.
"MMPs play a significant role in wrinkle formation, a characteristic of photoaging."[26]
If the intensity is too high, particularly if it is causing heat, then it would have negative effects on the skin by triggering ROS and MMP-1 in the skin.
Skincare Dosing Examples:
One article proposes using an LED mask with intensity 6.4 mW/cm^2 for 21 minutes to get 8.02 J/cm^2 dose twice a week for 4 weeks. [27]
Another article notes that typical face mask intensities range from 1 to 22 mW/cm^2 used for 10-12 minutes. The trial used 22mW/cm^2 for 12 minutes dosed twice a week for 3 months with a minimum spacing between doses of 72 hours. [1]
This article also agrees that proper intensity (mW/cm^2) is often more important than just calculated "dose" (J/cm^2) especially for skincare. Which we covered extensively in a previous blog.
"Indeed, the power density is related to the results of skin efficiency rather than considering the overall fluence delivered and has given rise to a patent." [1]
A study using the Omnilux For Men mask on 7 male participants with 3-5 treatments per week for 10 minutes per treatment for 6 weeks. The participants observed improvement in facial lines and wrinkles. [22]
The Omnilux LED Mask used in the study reports a peak intensity of 35mW/cm^2 as they designed the device with proper dosing in mind (which means proper intensity and exposure time). [Link]
The famous Celluma LED Skincare Device reports in their FDA Clearance document an intensity of 6.5 mW/cm^2 for 1800 seconds (30 minutes) for 11.7 J/cm^2 for 3 treatments per week. [Link]
So a reasonable dose for skincare is usually between 2 to 35mW/cm^2 for 10-30 minutes. Where higher intensities would be correlated with the higher possibility of negative outcomes, even if you compensate the exposure time and "dose" of J/cm^2.
The induction of ROS and MMPs by excessive intensities of Near-Infrared light and/or heat may play a role in skin volume loss by triggering a loss of collagen production and increased wrinkles. This may be perceived as a "facial fat loss" from Red Light Therapy but is likely a degradation of other structures in the skin.
If consumers are using higher intensities than the science recommends, it will not be surprising that they discover adverse events that are not observed in properly designed studies.
LLLT Can Reduce Facial Puffiness - Moon Face
Facial puffiness may be correlated with perceived rounded features and youthfulness.
However, this may be brought on by fluid retention and inflammation of the face. This can be unknowingly "normal" for many people, as the modern diet and lifestyle and diseases may cause a chronic low-level inflammation of the face.
"Facial puffiness, caused by mild or normal fluid retention, commonly experienced by women, may not pose a health risk, but it can be a cause of cosmetic concern." [28][Link]
The condition called "moon face" occurs when facial puffiness is brought about by certain medications or conditions. [29][30]
Photobiomodulation is well known to reduce inflammation, reduce edema (swelling and water retention), and also promotes lymph drainage and circulation.
For example, LLLT is often employed to reduce fluid volume and edema in Lymphedema as noted in these 3 studies.[31][32][33]
"There are reports of stimulation of local fluid circulation,20 and stimulatory effects on lymphatic vessels,9 perhaps in response to increased fluid mobility in laser-irradiated tissues."[31]
Another example is that LLLT is often used to reduce pain and facial swelling (edema) from third molar extraction (wisdom teeth removal). [34][35]
When PBM is applied to an inflamed face with fluid retention, there may be a perceived reduction in facial volume. It may even be rapid and occur after only a few doses.
While this is a beneficial result for overall wellness; but may be contrary to some cosmetic goals that aim to preserve facial volume. Even if the volume was unknowingly being maintained by inflammatory mechanisms.
Sunlight and Skin Aging
Before we transition into weight loss and abdominal contouring, we should note the role Sunlight plays on facial aging and weight management.
Photoaging is the effect of light causing accelerated skin aging particularly on the face. The primary factors of photoaging are from Sunlight, particularly the UV, Blue, and Infrared on the face. As noted by the following quote from a 2021 article:
"Importantly, photoaging of human skin is not only caused by ultraviolet (UV) B and A radiation, but is also the consequence of exposure to wavelengths beyond the UV spectrum. These include visible, i.e. blue light (400-440 nm) as well as the short part of infrared radiation, i.e. IRA (760-1200 nm)." [36]
Even though Near-Infrared (IR-A) is mentioned here, this is why the previous articles recommend NIR intensities equivalent or below the intensity of sunlight ~35mW/cm^2 in that wavelength range of the spectrum.
In addition to the induction of wrinkles, excess sun exposure has been shown to affect facial fat distribution.
"On sun-exposed areas such as the face, aging also causes a redistribution of fat between subcutaneous facial compartments, which is an important part of perceived facial aging (Rohrich and Pessa 2007, 2008)." [37]
Another article makes clear:
"Indeed UV exposure seems to be responsible for 80% of visible facial aging signs." [38]
Thus, often the advisement from skincare professionals to find safe ways to reduce UV, Blue Light, and Infrared Heat exposure to the face.
Aging and Obesity
Increasing age is often correlated with increased obesity. As a 2023 review article titled "Aging and Obesity" describes the many aspects of this epidemic:
"The propensity to develop excess adiposity with aging is multifactorial, mediated by adipose tissue dysfunction, changes in energy intake and expenditure, and hormonal changes." [39]
A 2010 review article also describes the association of age with fat.
"In addition, increasing age is associated with increased accumulation of visceral fat. This increase is dramatic in women, as shown in Figure 1, almost quadrupling between the ages of 25 and 65 years, adapted from Hunter et al 19." [40]
This shows that we have opposing goals - with aging we need to combat body fat accumulation while reducing facial fat loss.
Sunlight and Obesity
Sunlight has many roles to play in preventing and managing obesity.
A 2016 Review Article looked at the mechanisms of sunlight on managing obesity and related metabolic disorders. They note the production of Vitamin D and Nitric Oxide as playing a key role particularly from the Ultraviolet (UV) exposure.
"These observations suggest that regular exposure to safe levels of sunlight could be an effective means of reducing the burden of obesity." [41]
A 2024 article titled "From the Sun to the Cell: Examining Obesity through the Lens of Vitamin D and Inflammation" explores these mechanisms further.
As is often noted, low Vitamin D levels are often found in obese people. Which further exacerbates the metabolic dysfunction.
"Vitamin D deficiency is a frequent finding in overweight or obese people." [42]
However, this correlation works both ways. Low Vitamin D may contribute to weight gain through metabolic dysfunction and inflammation. Conversely, Vitamin D is stored in the fat and removes Vitamin D availability causing even lower levels measured in the blood. Thus creating a downward spiral. The intervention is that Obese people may need higher Vitamin D supplementation to break the cycle until they return to a more normal weight.
"The trapping hypothesis proposes that fat cells “capture” vitamin D, preventing it from being efficiently metabolized or used by the body. This finding may explain the relationship between obesity and reduced levels of circulating vitamin D, as well as the need for individuals with obesity to take higher dosages of vitamin D to attain comparable blood levels to those with lower adiposity [11,17,24,26,27]." [42]
Another article makes clear the importance of UltraViolet light for fat loss.
"Ultraviolet radiation from sunlight exposure increases endogenous production of vitamin D with subsequent reduction in adiposity (14). " [43]
It is known that Red and Near-Infrared light does not stimulate the synthesis of Vitamin D. Only Ultraviolet light has a direct effect on Vitamin D production.
However, one small human study used LLLT on the feet and legs of patients with Diabetes, Vitamin D deficiency, and Neuropathy. They found a significant increase in blood serum Vitamin D levels (9.91ng/ml to 16.81ng/ml average) after 4 weeks of treatment. Perhaps promoted by an indirect mechanism like liberating Vitamin D from fat stores or reducing inflammation. [44]
Again we have opposite goals. We need to manage the Sunlight/UV to the face to prevent photoaging, while still getting adequate Sunlight/UV to the body for Vitamin D, Nitric Oxide, and Metabolism. As well appreciating that Sunlight provides a large percentage of its spectrum in Red and Near-Infrared for free.
Bright Light Therapy, Sleep, and Obesity
Sleep is very valuable for weight loss and metabolic function. The sleep hormone melatonin is related to obesity for it's antioxidant properties. [45]
Poor sleep is correlated to obesity particularly for being known to cause increased appetite and food consumption. This is often assumed to be increased energy required for being awake longer, and from dysregulation of hunger hormones ghrelin, leptin, and insulin. [46]
Preliminary research shows poor sleep may affect GLP-1 secretion in a negative way. [46] [47]
As the following two quotes make clear, poor sleep quality and short sleep durations are strongly correlated with obesity.
"The causality of sleep curtailment and obesity can be attributed to neuroendocrine changes, which are related to appetite disorders [11,12]." [46]
And:
"Short sleep duration and later sleep timing have been linked to higher BMI in multiple studies [9], [10], [11], [12], [13], [14]." [48]
Thus it has been clear that poor sleep is often responsible for weight gain, and improving the quality of sleep can be vital for weight loss.
Bright Light Therapy is the exposure of bright lights to the eyes particularly in the mornings. It has been conventionally recommended for Seasonal Affective Disorder (SAD), but now is being researched for many more diseases as it improves circadian rhythms and sleep.
One study found that bright light therapy helped manage fat loss and appetite in women.
"In a study by Danilenko and colleagues, exposure to at least 45 minutes of morning light (between 6–9 am at 1300 lux) for 3 weeks in obese women resulted in reduced body fat and appetite " [49]
Thus, reinforcing the recommendations for "morning sunlight" for overall heath and wellness, circadian rhythms, sleep, melatonin production, and we know now this can be a powerful tool for managing weight.
Light at Night vs Sleep and Obesity
Excessive light at night, particularly the blue light spectrum from modern screens and white LEDs, also contributes to poor sleep quality and reduced melatonin production.
"This could explain why large epidemiological studies have shown a direct relationship between obesity and light exposure at night, even when adjusting for other factors such as sleep duration and physical activity [27]." [50]
A 2023 survey study found a strong correlation between Artificial Light At Night (ALAN) and childhood obesity. They specifically note that ALAN is an endocrine disruptor.
"We emphasize that ALAN should and likely will be a focus for children and adolescents with overweight and obesity." [51]
Weight loss interventions should include the usage of dim lights in the evenings, reduced exposure to blue light spectrum in the evenings, and total darkness during sleep.
Anything But Exercise:
Non-invasive body contouring is a popular method of non-surgical and non-drug related fat reduction, particularly of the abdominal region.
The list of non-invasive body contouring and fat reduction techniques often include:
- Radiofrequency
- High Intensity Focused Ultrasound (HIFU)
- Laser lipolysis
- High-Intensity Focused Electromagnetic Field
- Cryolipolysis (i.e. CoolSculpting)
- Low Level Laser Therapy
- Extracorporeal shockwave therapy
- Vibration Exercise and Weight Reduction
These are various electromagnetic-energy-based techniques, mechanical or acoustic vibrations, and cold.
Of note for this blog, the Radiofrequency and Laser Lipolysis use high intensity electromagnetic frequencies to cause heat-based destruction of fat cells.
"The principle of this non-invasive method is based on raising the temperature of adipocytes to the threshold of cell death, i.e., 42~47 °C; their complete decomposition occurs at 50~65 °C. With the accumulation of heat, the adipocytes are irreversibly damaged by the formation of transient micropores in their membranes, followed by the release of intracellular lipids. As with cryolipolysis, the inflammation leads to the removal of dead cells [21,22]." [52]
Radiofrequency treatments can be used to specifically target facial fat. [53] When RF is used on the face for other reasons like facial rejuvenation, there is a small risk of causing unwanted facial fat loss. [54]
A 1060nm laser is often employed for body contouring treatments. This is a deep penetrating wavelength, and one article reports the intensity as 1.2 W/cm^2, which is 1,200 mW/cm^2. [55][56][57]
The 1060nm laser treatment has been used for submental fat reduction. This is the fat under the chin sometimes accumulating into the "double-chin" condition. With intensity up to 1,400mW/cm^2 they also note agreement that 20-25 minutes of treatment is ideal for the best effects. [58]
One study combined 1060nm high intensity laser with 635nm LLLT as they noted there could be synergistic for fat mobilization with LLLT and the destruction from the high intensity laser. The laser intensity was up to 1,400 mW/cm^2 for the abdominal fat and up to 2,350mW/cm^2 for the under-chin fat. The LLLT intensity was 36.3 mW/cm^2. [59]
So we can establish that high-intensity laser causing heat damage is becoming more common for both under-chin and abdominal fat treatments. This may be good reason to avoid excessive intensities that cause heat for facial treatments if avoiding fat loss is a goal.
Red Light Therapy for Spot Fat Reduction:
Low Level Laser Therapy (Photobiomodulation, Red Light Therapy) is included in 4 different reviews of non-invasive body contouring and fat reduction articles. [52][60][61][62]
In contrast to the heating or cooling therapies, properly used LLLT/PBM has no significant effect on tissue temperature.
"Applying LLLT for fat removal has no observable consequence on surrounding tissues and does not increase tissue temperature." [52]
A 2023 review article on Non-Invasive Body Contouring notes that the mechanisms for LLLT to cause fat loss are still controversial. [60]
However, the review articles discuss how the effects of LLLT are subtle and require a combination of different treatments.
"Although there are some evidences, which show the effects of LLLT on reducing fat in combination with liposuction, the evidences for the effects of this method as a stand-alone procedure, are not sufficient (56). " [52]
The 2023 review article also comments that LLLT/PBM must be combined with aerobic exercise for the benefits of weight loss or body contouring. [60]
Photobiomodulation Fat Loss Mechanisms:
One article summarized the primary theory for the mechanism that Red Light Therapy can promote fat loss.
"Recently, low-level laser therapy was reported to "liquefy" or release stored fat in adipocytes by the opening of specialized yet not identified cell membrane-associated pores after a brief treatment." [63]
A 2013 article on Low Level Laser Therapy for Fat Reduction reviews all of the articles and potential mechanisms at the time. They describe the mechanism as the adipocytes (cells that store fat) developing micropores that release the fat. Another proposed mechanism is that LLLT activates ATP metabolism and enzymes that facilitate lipolysis. [64]
Despite the proposed mechanism of releasing lipids from the adipocytes, several studies confirmed no impact on blood lipids and possibly even a reduction in blood lipid markers.[64] Which appears to be paradoxical to the proposed mechanism of action.
There appears to be a missing step in this mechanism. When the lipids are released, where do they go? How exactly do they get metabolized or burned off? Why are lipids not found in the blood after treatments?
Photobiomodulation Weight Reduction:
While the studies below confirm some "body contouring" benefits with statistical significance, it is clear that only a small amount of body weight is lost in the process. The overall weight loss is not competitive with standard diet and exercise, and is far away from the kind of weight loss seen in Semaglutide drugs.
Most LLLT studies on body contouring focus on circumference measurement reductions from various key areas, although the actual weight loss is statistically insignificant or so small that it is not clinically relevant.
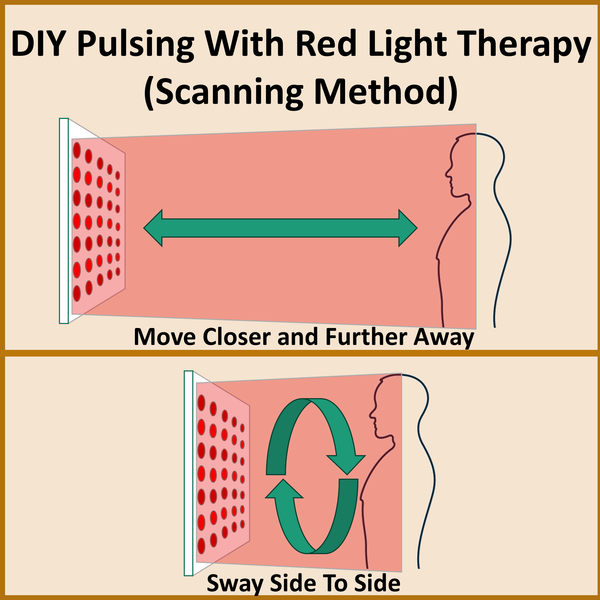
The most popular wavelength for fat reduction in 2013 was 635nm delivered by a 17mW laser in a scanning mode for 40 minutes for about 1-4 J/cm^2 per treatment. Treatments were performed 3 times a week with at least 1 day off between treatments. [64]
One article with this treatment found positive results in body circumference and patient satisfaction, there was no statistically significant change in BMI (Body Mass Index, the ratio of the weight to height). [65]
Another 2013 study found a mean weight reduction of 1.24 lbs (0.56 kg) with statistically significant body circumference changes. [66]
A 2016 study with similar parameters recorded an average weight loss of 0.7 kg (1.5lbs) that was statistically significant. However, the authors comment that this amount of weight loss is "not clinically meaningful". [67]
A 2020 LLLT article have used Green 535nm wavelength from a 17mW laser for 30 minutes. They tested doing treatments twice a week versus three times a week and found better results with twice a week treatments.[68]
They report 25% of patients in the 2x per week group had a >3% reduction from their initial body weight after 6 weeks of treatment. Only 15% of that group maintained that weight reduction after a 26 week checkup. [68] This is a suspiciously odd way the authors chose to present the weight loss data. For example, this means that the vast majority 75% of participants had less than 3% weight loss. It may even be possible that some participants gained weight, but the way they present the data hides that from us.
Notably, they still cite the same mechanisms we discussed earlier for Green 535nm as the Red 635nm. However, since we know that Green has significantly less penetration than Red, we must start to assume that there are more systemic mechanisms involved with these new trials using Green.
A recent 2024 article also used 17mW green lasers for an improvement in body contours, but no significant difference in body weight or BMI.
"Our results showed that 6 treatment sessions with a PBM-based device significantly decreased local obesity in abdomen, buttock, thigh, and arm areas in Middle Eastern participates without significant change in BMI." [85]
They also recommend that LLLT should be combined with exercise or vibration therapy.
"It should be associated with techniques that promote beta-oxidation, such as physical exercise and vibration platform (13)." [85]
Even though some of these results are statistically significant, the magnitude of weight loss is quite small from Red Light Therapy alone. Which begs the question that if they are seeing "Fat Reduction" in targeted spots, why is there insignificant weight loss? Is the fat simply being redistributed, or is there a commensurate increase in lean mass like a body recomposition effect?
Fat Loss Parameters for Face vs Abdominal Fat:
The 2013 review article on LLLT for Fat Reduction leaves a comment on the possibility of facial fat loss:
'Lastly, it is worthwhile to note that LLLT parameters used for facial skin rejuvenation and acne treatments are close to the ones used in fat reduction [84,85]. Therefore, it is possible that facial volume loss may occur while using LLLT. " [64]
However, this is contrary to their other conclusions that LLLT alone has not been shown to promote significant fat loss without other interventions like diet, exercise, supplements, or liposuction.
A 2017 article explains that facial fat cells have different characteristics and metabolism than abdominal fat cells.
"Recently, it was demonstrated that human facial preadipocytes (adipose derived stem cells) exhibit very different properties compared with abdominal preadipocytes.13" [69]
Meaning that in a hypothetical situation; even if we find the perfect PBM parameters for abdominal fat loss, those exact parameters would likely not work the same on facial fat cells.
For example the earlier study with the high-intensity 1060nm laser used 1,400 mW/cm^2 on the abdomen and 2,350mW/cm^2 for the under-chin fat. [59] We could assume the facial fat is more resilient to these treatments and required a higher intensity, perhaps as an adaptation to sunlight exposure being predominantly on the face.
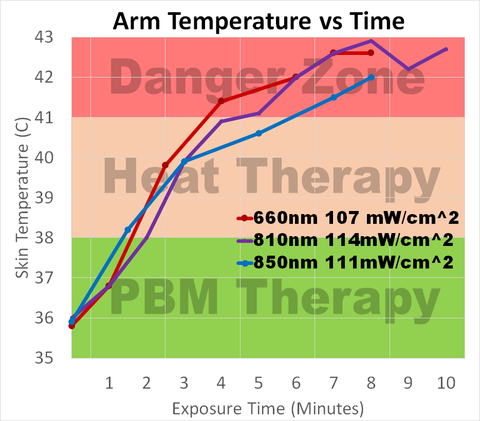
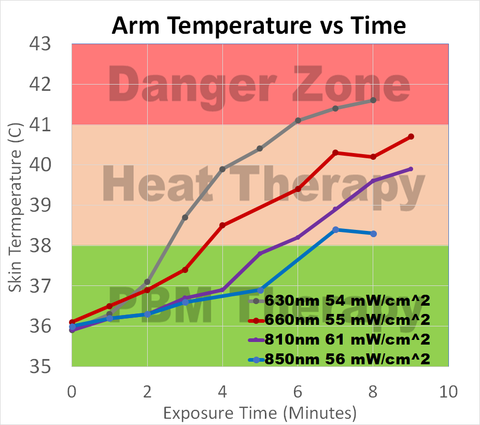
Fun Fact: The Face as a Heat Sensor
The face has been found to be 2-5 times more sensitive to feeling heat than other parts of the body.
"During local warming (W+4), the face was 2, 3 and 5 times more thermosensitive than the lower limb, upper limb and limb extremity segments" [70]
This would explain why we can feel heat on our face from a red light therapy panel, but at the exact same distance and intensity not feel much heat on the rest of the body.
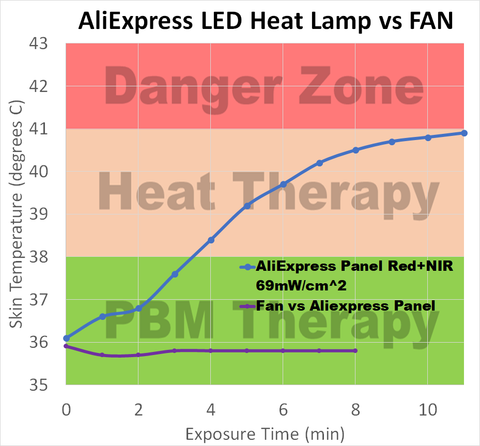
We would speculate that this could be a powerful evolutionary sensor for the human to seek shade when feeling radiant heat on the face, particularly to protect from potential photodamage or photoaging. Feeling radiant heat on the face from a red light therapy device is a good indication that the intensity should be reduced.
Red Light Therapy Increases Fat and Weight Gain:
Several studies have shown that Red Light Therapy can actually increase weight, fat accumulation, and adipose tissue.
According to Dr. Hamblin while being interviewed by Max Lugavere on The Genius Life Podcast:
"It combines very well with exercise. Especially because a lot of people are interested in weight loss. And if you just try using light therapy alone to lose weight, it's probably not gonna work. In fact, we did an animal study and the rats had got a high-fat diet plus Photobiomodulation actually gained more weight than just the high-fat alone. So it stimulated the weight gain but if they did high-fat diet, exercise, and photobiomodulation then they lost more weight with the addition of the light."
https://www.maxlugavere.com/podcast/129-michael-hamblin
From what Dr. Hamblin notes, we could actually increase weight gain with poor diet combined with Photobiomodulation. Only when exercise is added into the protocol that the combination of PBM and exercise leads to weight loss.
The rodent study that Dr. Hamblin referenced makes this comment that the sedentary (no-exercise) PBM group gained more weight than the Control group that didn't get any PBM.
"In the LLLT sedentary groups (SNL and SHL), the relative weight of EPI was greater than respective controls (SN and SH)." [71]
The combination of Poor Diet + LLLT led to increased weight gain compared to Poor Diet alone. Only the Poor Diet + LLLT + Exercise group were able to reap the weight loss benefits from this combination.
"The combination of exercise and LLLT increased the benefits of exercise alone. However, LLLT without exercise tended to increase body weight and fat content."[71]
One human study attempted to use LLLT for fat loss and ended up with this result:
"we have observed that in 8 out of 17 patients LLLT increased adipose tissue thickness." [72]
They conducted the study as a split-abdomen design. Meaning they only treated one side of the abdomen and the opposite side was untreated as it's own "control". Similar to a split-face design for skincare clinical trials.
While the treated side had, on average, an extremely modest 0.07 cm reduction as measured by ultrasound, the untreated side on average gained 0.16 cm. This is a common concern of spot fat reduction treatments that the fat may simply be redistributed to a different part of the body. [72]
On average the participants lost 1.25 kg (2.75 lbs), but this was not statistically significant. [72]
The same study notes that the prominent mechanism of localized fat liquification fails to explain these results. They propose that fat reduction from LLLT is likely though systemic (indirect) mechanisms. [72] This again is good news for usage of Red Light Therapy on the face, as it likely does not cause the spontaneous mobility of fat from the facial fat stores.
Improperly applied red light therapy to humans can increase fat gain. They recommend that exercise is essential for using Red Light Therapy for fat and weight loss.
"Under this model, the combination of LLLT and aerobic exercise is crucial for its efficacy in the reduction of subcutaneous adipose tissue thickness." [72]
The 2013 review article notes a mechanism that LLLT promotes adipocyte survival during fat grafts. So this could be a preliminary observation that LLLT can promote fat cell proliferation.
"Since adipose cells were shown to be alive and were able to recover their anatomy, application of LLLT could increase the number of viable adipocytes that survive [82,83]." [64]
This is good news for the people concerned about facial fat loss. Since Photobiomodulation may actually increase weight gain and stimulate fat tissue production depending on the parameters and lifestyle.
Naturally this information unfavorable for the people using Red Light Therapy for weight loss, and it reinforces the point that PBM should be combined with proper diet, exercise, and other lifestyle changes to promote fat reduction. If implementing PBM alone or improperly then it would actually risk increasing weight gain.
Red Light Therapy Plus Exercise
By now it is clear that Red Light Therapy should be combined with exercise for the goals of weight loss and fat reduction. So lets take a look at a few studies that combined LLLT and Exercise in humans.
One study with 62 obese women used 64 Lasers with 808nm and 100mW per laser for 8 minutes. The lasers were incorporated into flexible wraps and treated the abdomen, limbs, and glutes. It was 6,411 Total Joules per session.[73]*
Exercise was performed 3 times a week for 4 months and included 30 minutes of aerobic exercise and 30 minute of resistance training. The laser treatment occurred after each exercise session. [73]
The placebo group received the same Exercise but no LLLT. The Exercise-Only group lost on average 2.7 kg (6 lbs) and the Exercise+LLLT group lost 5.2 kg (11.4 lbs). The Percent Fat Mass was reduced by 1.8 % and 2.1% in the placebo and treatment groups, respectively. [73] This is a good result for the concept that Red Light Therapy and exercise can promote superior weight loss compared to exercise alone.
"LLLT associated with concurrent exercise (aerobic plus resistance training) potentiates the exercise effects of decreasing the cardiometabolic risk factors in obese woman." [73]
Another study from the same research group used a similar exercise and LLLT protocol. However, this time the results showed similar reductions in body weight, BMI, and body fat percentage in both the Exercise-Only and Exercise+LLLT groups. Although they note the Exercise+LLLT group showed superior improvements in inflammatory markers.
"Nevertheless, it is important to note that in both analyzed groups, the BMI, body mass, and body fat presented similar changes, considering delta values after 20 weeks of LLLT associated with physical exercise training." [74]
So with this study we did not see a significant difference in weight loss or body composition between the two groups. [74] **
A 2011 study used non-contact LED panels while simultaneously exercising on a treadmill for 45 minutes. There were 2 LED panels on each side targeting the thighs, hips, and glutes. Wavelength was 850nm and the devce was positioned 15cm away with 39 mW/cm^2 intensity landing on the skin. The placebo group only received treadmill training. While they found statistically significant improvements in body circumference and the appearance of cellulite, there was no statistically significant difference in overall weight loss, body fat%, fat mass, or lean mass. [75]
A similar study from the same researchers also found improvement in health markers but no significant differences in body weight or body composition between the groups. [76]
So only 1 out of 4 articles we could find combining LLLT + Exercise did the LLLT led to improved weight loss compared to Exercise alone.
Red Light Therapy for Increased Muscle Growth:
Body recomposition is a large factor in metabolic health and obesity management. Even if body weight stays the same, if the % lean mass increases and the % fat mass decreases - then that is a highly desirable outcome.
One study performed a strength training program 3 days a week for 12 weeks. One twin received an 850nm LED pad treatment for 15 seconds and 75 Total Joules on the thighs after each training session. [77]
The study found the exercise-only twin gained 5% muscle volume, and the Exercise+LLLT twin gained a 20% increase in muscle volume. Thus demonstrating superior muscle hypertrophy from the LLLT treatment. [77]
It would be interesting to see more of the LLLT studies on athletes monitor body weight and body composition. For example one LLLT study used a DEXA scan on the athletes before the trial to establish some baseline metrics, but did not take a DEXA scan after the protocol finished. [78]
Indirect Ways Red Light Therapy Can Support Weight Loss
By now it is clear that even if weight loss from Red Light Therapy can be statistically significant, the magnitude of weight loss from Red Light Therapy is quite small.
However, Red Light Therapy can certainly support a weight loss protocol in many indirect ways.
- It can reduce delayed onset muscle soreness (DOMS) which in-turn will promote better compliance to an exercise routine. [79]
- Red Light Therapy can improve sleep quality, which as we mentioned earlier plays a big role in weight management. [80][81]
- Red Light Therapy has been shown to stabilize blood sugar response and insulin levels. Which can improve metabolic health as well as potentially lead to more stable energy levels and appetite regulation. [82] [83]
Conclusions:
Non-Thermal Red & NIR Light Therapy does not appear to make a large impact on fat or body weight. Both in the face or abdominal regions.
While some studies show a statistically significant improvement in body circumpherence measurements, it is clear the Red Light Therapy should be combined with other complimentary weight loss techniques particularly exercise. However, even when we examine the studies that combine LLLT and exercise, there is not a large difference in weight loss compared to exercise alone.
Depending on the parameters and context, it appears equally likely that Red Light Therapy could support weight gain just as much as it can support weight loss. As always, showing a contradictory biphasic nature that must be further investigated.
Incorporating Bright Light Therapy and Ultraviolet exposure will also play a large role in obesity management. Both of these can be gotten for free from Sunlight, in addition to the Red/NIR in the sunlight spectrum.
High intensity laser treatments are already employed in body contouring and chin fat reduction, with seemingly more consistent results and better defined mechanisms than LLLT. So there is a bright future for using many forms of light therapy for managing obesity.
Since Red Light Therapy currently shows minimal direct impact on body fat, this should assuage some fears that it can cause facial fat loss. Overall, Red Light Therapy can certainly be used to support facial rejuvenating and anti-aging goals, often with an improvement in the appearance of facial volume.
Footnotes
* Since the spot size is extremely small of 0.0169 cm^2, the intensity was 6,000mW/cm^2 and energy density 2,880 J/cm^2 with 8 minutes per area. This is how it is quite easy for influencers to cherry pick laser studies to promote high intensity LED panels. Low Level Lasers often deliver low power outputs and low energy doses, but have extremely high "density" due to having small spot sizes of 0.0169cm^2. Naturally it is reckless and irresponsible for influencers to imply that one needs the intensity of a laser to engulf a large area of the body for effectiveness, and shows a lack of technical understanding of the intricacies of these parameters.
https://pubmed.ncbi.nlm.nih.gov/26398817/
** Unlike the prior study, this study also monitored the Lean Mass % (i.e. muscle mass percentage). During weight loss it is vital to reduce fat and at least preserve muscle. This study showed an average increase of 3.94% for the treatment group and an increase of 6.16% in the placebo group. With a change in lean/fat ratio of 0.20 and 0.25 for the treatment and placebo groups, respectively. This indicates a more favorable change in muscle for the Exercise-only group than the Exercise + LLLT group.
https://pubmed.ncbi.nlm.nih.gov/25958170/
References:
[1]
Couturaud V, Le Fur M, Pelletier M, Granotier F. Reverse skin aging signs by red light photobiomodulation. Skin Res Technol. 2023 Jul;29(7):e13391. doi: 10.1111/srt.13391. PMID: 37522497; PMCID: PMC10311288.
[2]
Hernández-Bule ML, Naharro-Rodríguez J, Bacci S, Fernández-Guarino M. Unlocking the Power of Light on the Skin: A Comprehensive Review on Photobiomodulation. Int J Mol Sci. 2024 Apr 19;25(8):4483. doi: 10.3390/ijms25084483. PMID: 38674067; PMCID: PMC11049838.
[3]
Li K, Meng F, Li YR, Tian Y, Chen H, Jia Q, Cai H, Jiang HB. Application of Nonsurgical Modalities in Improving Facial Aging. Int J Dent. 2022 Feb 24;2022:8332631. doi: 10.1155/2022/8332631. PMID: 35251183; PMCID: PMC8894069.
[4]
Szczerkowska-Dobosz A, Olszewska B, Lemańska M, Purzycka-Bohdan D, Nowicki R. Acquired facial lipoatrophy: pathogenesis and therapeutic options. Postepy Dermatol Alergol. 2015 Apr;32(2):127-33. doi: 10.5114/pdia.2014.40971. Epub 2015 Mar 30. PMID: 26015783; PMCID: PMC4436232.
[5]
Kruglikov IL, Scherer PE. Skin aging: are adipocytes the next target? Aging (Albany NY). 2016 Jul;8(7):1457-69. doi: 10.18632/aging.100999. PMID: 27434510; PMCID: PMC4993342.
[6]
Swift A, Liew S, Weinkle S, Garcia JK, Silberberg MB. The Facial Aging Process From the "Inside Out". Aesthet Surg J. 2021 Sep 14;41(10):1107-1119. doi: 10.1093/asj/sjaa339. PMID: 33325497; PMCID: PMC8438644.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8438644/
[7]
de Jager S, Coetzee N, Coetzee V. Facial Adiposity, Attractiveness, and Health: A Review. Front Psychol. 2018 Dec 21;9:2562. doi: 10.3389/fpsyg.2018.02562. PMID: 30622491; PMCID: PMC6308207.
[8]
Tay W, Quek R, Kaur B, Lim J, Henry CJ. Use of Facial Morphology to Determine Nutritional Status in Older Adults: Opportunities and Challenges. JMIR Public Health Surveill. 2022 Jul 18;8(7):e33478. doi: 10.2196/33478. PMID: 35849429; PMCID: PMC9345026.
[9]
Flament F, Bazin R, Laquieze S, Rubert V, Simonpietri E, Piot B. Effect of the sun on visible clinical signs of aging in Caucasian skin. Clin Cosmet Investig Dermatol. 2013 Sep 27;6:221-32. doi: 10.2147/CCID.S44686. PMID: 24101874; PMCID: PMC3790843.
[10]
Singh G, Krauthamer M, Bjalme-Evans M. Wegovy (semaglutide): a new weight loss drug for chronic weight management. J Investig Med. 2022 Jan;70(1):5-13. doi: 10.1136/jim-2021-001952. Epub 2021 Oct 27. PMID: 34706925; PMCID: PMC8717485.
[11]
The rise of “Ozempic Face”: Analyzing trends and treatment challenges associated with rapid facial weight loss induced by GLP-1 agonists
Mansour, Meghan R.Hannawa, Olivia M.Yaldo, Marissa M.Nageeb, Emmanuel M.Chaiyasate, Kongkrit et al.
Journal of Plastic, Reconstructive & Aesthetic Surgery, Volume 96, 225 – 227
[12]
Papoian V, Mardirossian V, Hess DT, Spiegel JH. Effects of Bariatric Surgery on Facial Features. Arch Plast Surg. 2015 Sep;42(5):567-71. doi: 10.5999/aps.2015.42.5.567. Epub 2015 Sep 15. PMID: 26430627; PMCID: PMC4579167.
[13]
O’Neill, Elizabeth S. MD, MPH*; Wiegmann, Aaron L. MD, MS*; Parrella, Naomi MD†; Pittman, Troy MD‡; Hood, Keith MD*; Kurlander, David MD*. Injectable Weight Loss Medications in Plastic Surgery: What We Know, Perioperative Considerations, and Recommendations for the Future. Plastic & Reconstructive Surgery-Global Open 12(1):p e5516, January 2024. | DOI: 10.1097/GOX.0000000000005516
[14]
Zainab Ridha, Sabrina Guillen Fabi, Raheel Zubar, Steven H Dayan, Decoding the Implications of Glucagon-like Peptide-1 Receptor Agonists on Accelerated Facial and Skin Aging, Aesthetic Surgery Journal, 2024;, sjae132, https://doi.org/10.1093/asj/sjae132
[15]
Bikou A, Dermiki-Gkana F, Penteris M, Constantinides TK, Kontogiorgis C. A systematic review of the effect of semaglutide on lean mass: insights from clinical trials. Expert Opin Pharmacother. 2024 Apr;25(5):611-619. doi: 10.1080/14656566.2024.2343092. Epub 2024 Apr 18. PMID: 38629387.
[16]
Martinelli A, Andreo L, Alves AN, Terena SML, Santos TC, Bussadori SK, Fernandes KPS, Mesquita-Ferrari RA. Photobiomodulation modulates the expression of inflammatory cytokines during the compensatory hypertrophy process in skeletal muscle. Lasers Med Sci. 2021 Jun;36(4):791-802. doi: 10.1007/s10103-020-03095-y. Epub 2020 Jul 7. PMID: 32638240.
[17]
Rodrigues CP, Jacinto JL, Roveratti MC, Merlo JK, Soares-Caldeira LF, Silva Ribeiro A, Nunes JP, Junior EO, Aguiar AF. Effects of Photobiomodulation/Laser Therapy Combined With Resistance Training on Quadriceps Hypertrophy and Strength, and Postural Balance in Older Women: A Randomized, Triple-Blinded, Placebo-Controlled Study. J Geriatr Phys Ther. 2022 Jul-Sep 01;45(3):125-133. doi: 10.1519/JPT.0000000000000313. Epub 2021 May 28. PMID: 34054079.
[18]
Kumar P, Umakanth S, N G. Photobiomodulation therapy as an adjunct to resistance exercises on muscle metrics, functional balance, functional capacity, and physical performance among older adults: A systematic scoping review. Lasers Med Sci. 2024 Sep 3;39(1):232. doi: 10.1007/s10103-024-04177-x. PMID: 39225877; PMCID: PMC11371873.
[19]
Vatansever F, Rodrigues NC, Assis LL, Peviani SS, Durigan JL, Moreira FM, Hamblin MR, Parizotto NA. Low intensity laser therapy accelerates muscle regeneration in aged rats. Photonics Lasers Med. 2012 Oct 1;1(4):287-297. doi: 10.1515/plm-2012-0035. PMID: 23750328; PMCID: PMC3671618.
[20]
Graeme Ewan Glass, Photobiomodulation: The Clinical Applications of Low-Level Light Therapy, Aesthetic Surgery Journal, Volume 41, Issue 6, June 2021, Pages 723–738, https://doi.org/10.1093/asj/sjab025
[21]
Mota LR, Duarte IDS, Galache TR, Pretti KMDS, Neto OC, Motta LJ, Horliana ACRT, Silva DFTD, Pavani C. Photobiomodulation Reduces Periocular Wrinkle Volume by 30%: A Randomized Controlled Trial. Photobiomodul Photomed Laser Surg. 2023 Feb;41(2):48-56. doi: 10.1089/photob.2022.0114. PMID: 36780572.
[22]
Mineroff J, Austin E, Feit E, Ho A, Lowe B, Marson J, Mojeski J, Wechter T, Nguyen JK, Jagdeo J. Male facial rejuvenation using a combination 633, 830, and 1072 nm LED face mask. Arch Dermatol Res. 2023 Nov;315(9):2605-2611. doi: 10.1007/s00403-023-02663-w. Epub 2023 Jul 7. PMID: 37418018.
[23]
Bragato, Erick Frank Postgraduatea,*; Pires, Jefferson André Postgraduatea; Momolli, Marcos Postgraduatea; Guerra, Marina Bertoni Postgraduatea; Paisano, Adriana Fernandes PhDa; Ferrari, Raquel Agnelli Mesquita PhDa,b; Bussadori, Sandra Kalil PhDa; Motta, Lara Jansiski PhDa; Fernandes, Kristianne Porta Santos PhDa. Comparison of the effects of 2 frequencies of application of photobiomodulation on facial rejuvenation: Controlled, randomized, and double-blind clinical trial. Medicine 102(5):p e32514, February 3, 2023. | DOI: 10.1097/MD.0000000000032514
[24]
Barolet D. Near-Infrared Light and Skin: Why Intensity Matters. Curr Probl Dermatol. 2021;55:374-384. doi: 10.1159/000517645. Epub 2021 Oct 25. PMID: 34698043.
[25]
Lee YI, Lee SG, Jung I, Suk J, Baeg C, Han SY, Seo JY, Jung D, Jeon Y, Lee JH. Topical Application of Peptide Nucleic Acid Antisense Oligonucleotide for MMP-1 and Its Potential Anti-Aging Properties. J Clin Med. 2023 Mar 24;12(7):2472. doi: 10.3390/jcm12072472. PMID: 37048555; PMCID: PMC10095221.
[26]
Pittayapruek P, Meephansan J, Prapapan O, Komine M, Ohtsuki M. Role of Matrix Metalloproteinases in Photoaging and Photocarcinogenesis. Int J Mol Sci. 2016 Jun 2;17(6):868. doi: 10.3390/ijms17060868. PMID: 27271600; PMCID: PMC4926402.
[27]
Bragato EF, Pires JA, Momolli M, Guerra MB, Paisano AF, Ferrari RAM, Bussadori SK, Motta LJ, Fernandes KPS. Comparison of the effects of 2 frequencies of application of photobiomodulation on facial rejuvenation: Controlled, randomized, and double-blind clinical trial. Medicine (Baltimore). 2023 Feb 3;102(5):e32514. doi: 10.1097/MD.0000000000032514. PMID: 36749255; PMCID: PMC9902007.
[28]
Nkengne A, Robic J, Lua BL. Self-perceived and objective measurements of facial puffiness in Chinese women. Skin Res Technol. 2021 May;27(3):385-392. doi: 10.1111/srt.12955. Epub 2020 Oct 22. PMID: 33089925.
[29]
Clutter WE. Screening for Cushing's syndrome in an era of epidemic obesity. Mo Med. 2011 Mar-Apr;108(2):104-6. PMID: 21568231; PMCID: PMC6189156.
[30]
Hughes RA, Mehndiratta MM, Rajabally YA. Corticosteroids for chronic inflammatory demyelinating polyradiculoneuropathy. Cochrane Database Syst Rev. 2017 Nov 29;11(11):CD002062. doi: 10.1002/14651858.CD002062.pub4. PMID: 29185258; PMCID: PMC6747552.
[31]
Ahmed Omar MT, Abd-El-Gayed Ebid A, El Morsy AM. Treatment of post-mastectomy lymphedema with laser therapy: double blind placebo control randomized study. J Surg Res 2011; 165: 82-90.
[32]
Özçete ZA, Eyigör S. Kinesio taping and low-level laser therapy in breast cancer-related lymphedema in an arm with arteriovenous fistula for hemodialysis. Turk J Phys Med Rehabil. 2020 May 18;66(2):214-218. doi: 10.5606/tftrd.2020.3430. PMID: 32760900; PMCID: PMC7401690.
[33]
Mahram M, Rajabi M. Treatment of Lymphedema Praecox through Low Level Laser Therapy (LLLT). J Res Med Sci. 2011 Jun;16(6):848-51. PMID: 22091317; PMCID: PMC3214406.
[34]
Sigaroodi AK, Motevasseli S, Maleki D, Maleki D, Fard RS. Low-level laser and management of common complications after the mandibular third molar surgery: A double-blind randomized clinical trial. Dent Res J (Isfahan). 2023 Jan 18;20:14. PMID: 36820144; PMCID: PMC9937931.
[35]
Asutay F, Ozcan-Kucuk A, Alan H, Koparal M. Three-dimensional evaluation of the effect of low-level laser therapy on facial swelling after lower third molar surgery: A randomized, placebo-controlled study. Niger J Clin Pract. 2018 Sep;21(9):1107-1113. doi: 10.4103/njcp.njcp_38_18. PMID: 30156193.
[36]
Krutmann J, Berneburg M. Lichtalterung (Photoaging) der Haut: Was gibt es Neues? [Sun-damaged skin (photoaging): what is new?]. Hautarzt. 2021 Jan;72(1):2-5. German. doi: 10.1007/s00105-020-04747-4. Epub 2020 Dec 21. PMID: 33346860.
[37]
Rittié L, Fisher GJ. Natural and sun-induced aging of human skin. Cold Spring Harb Perspect Med. 2015 Jan 5;5(1):a015370. doi: 10.1101/cshperspect.a015370. PMID: 25561721; PMCID: PMC4292080.
[38]
Flament F, Bazin R, Laquieze S, Rubert V, Simonpietri E, Piot B. Effect of the sun on visible clinical signs of aging in Caucasian skin. Clin Cosmet Investig Dermatol. 2013 Sep 27;6:221-32. doi: 10.2147/CCID.S44686. PMID: 24101874; PMCID: PMC3790843.
[39]
Noemi Malandrino, Salman Z. Bhat, Maha Alfaraidhy, Rajvarun S. Grewal, Rita Rastogi Kalyani,
Obesity and Aging,
Endocrinology and Metabolism Clinics of North America,
Volume 52, Issue 2,
2023,
Pages 317-339,
ISSN 0889-8529,
ISBN 9780323939874,
https://doi.org/10.1016/j.ecl.2022.10.001.
(https://www.sciencedirect.com/science/article/pii/S0889852922000950)
Keywords: Obesity; Sarcopenia; Sarcopenic obesity; Aging
[40]
Hunter GR, Gower BA, Kane BL. Age Related Shift in Visceral Fat. Int J Body Compos Res. 2010 Sep 1;8(3):103-108. PMID: 24834015; PMCID: PMC4018766.
[41]
Fleury N, Geldenhuys S, Gorman S. Sun Exposure and Its Effects on Human Health: Mechanisms through Which Sun Exposure Could Reduce the Risk of Developing Obesity and Cardiometabolic Dysfunction. Int J Environ Res Public Health. 2016 Oct 11;13(10):999. doi: 10.3390/ijerph13100999. PMID: 27727191; PMCID: PMC5086738.
[42]
Popa, Alina Delia, Otilia Niță, Lavinia Caba, Andreea Gherasim, Mariana Graur, Laura Mihalache, and Lidia Iuliana Arhire. 2024. "From the Sun to the Cell: Examining Obesity through the Lens of Vitamin D and Inflammation" Metabolites 14, no. 1: 4. https://doi.org/10.3390/metabo14010004
[43]
Klinedinst BS, Meier NF, Larsen B, Wang Y, Yu S, Mochel JP, Le S, Wolf T, Pollpeter A, Pappas C, Wang Q, Allenspach K, Wang L, Russell D, Bennett DA, Willette AA. Walking in the Light: How History of Physical Activity, Sunlight, and Vitamin D Account for Body Fat-A UK Biobank Study. Obesity (Silver Spring). 2020 Aug;28(8):1428-1437. doi: 10.1002/oby.22852. Epub 2020 Jun 22. PMID: 32573118; PMCID: PMC7501143.
[44]
Anju M, Chacko L, Chettupalli Y, Maiya AG, Saleena Ummer V. Effect of Low Level Laser Therapy on serum vitamin D and magnesium levels in patients with diabetic peripheral neuropathy - A pilot study. Diabetes Metab Syndr. 2019 Mar-Apr;13(2):1087-1091. doi: 10.1016/j.dsx.2019.01.022. Epub 2019 Jan 18. PMID: 31336449.
[45]
Guan Q, Wang Z, Cao J, Dong Y, Chen Y. Mechanisms of Melatonin in Obesity: A Review. Int J Mol Sci. 2021 Dec 25;23(1):218. doi: 10.3390/ijms23010218. PMID: 35008644; PMCID: PMC8745381.
[46]
Liu S, Wang X, Zheng Q, Gao L, Sun Q. Sleep Deprivation and Central Appetite Regulation. Nutrients. 2022 Dec 7;14(24):5196. doi: 10.3390/nu14245196. PMID: 36558355; PMCID: PMC9783730.
[47]
Papaetis GS. GLP-1 receptor agonists, SGLT-2 inhibitors, and obstructive sleep apnoea: can new allies face an old enemy? Arch Med Sci Atheroscler Dis. 2023 Feb 28;8:e19-e34. doi: 10.5114/amsad/161170. PMID: 37153372; PMCID: PMC10161791.
[48]
Reid KJ, Santostasi G, Baron KG, Wilson J, Kang J, Zee PC. Timing and intensity of light correlate with body weight in adults. PLoS One. 2014 Apr 2;9(4):e92251. doi: 10.1371/journal.pone.0092251. PMID: 24694994; PMCID: PMC3973603.
[49]
Reid KJ, Santostasi G, Baron KG, Wilson J, Kang J, Zee PC. Timing and intensity of light correlate with body weight in adults. PLoS One. 2014 Apr 2;9(4):e92251. doi: 10.1371/journal.pone.0092251. PMID: 24694994; PMCID: PMC3973603.
[50]
Benedito-Silva AA, Evans S, Viana Mendes J, Castro J, Gonçalves BDSB, Ruiz FS, Beijamini F, Evangelista FS, Vallada H, Krieger JE, von Schantz M, Pereira AC, Pedrazzoli M. Association between light exposure and metabolic syndrome in a rural Brazilian town. PLoS One. 2020 Sep 18;15(9):e0238772. doi: 10.1371/journal.pone.0238772. PMID: 32946454; PMCID: PMC7500684.
[51]
Dang J, Shi D, Li X, Ma N, Liu Y, Zhong P, Yan X, Zhang J, Lau PWC, Dong Y, Song Y, Ma J. Artificial Light-at-Night Exposure and Overweight and Obesity across GDP Levels among Chinese Children and Adolescents. Nutrients. 2023 Feb 13;15(4):939. doi: 10.3390/nu15040939. PMID: 36839297; PMCID: PMC9961462.
[52]
Alizadeh Z, Halabchi F, Mazaheri R, Abolhasani M, Tabesh M. Review of the Mechanisms and Effects of Noninvasive Body Contouring Devices on Cellulite and Subcutaneous Fat. Int J Endocrinol Metab. 2016 Jul 3;14(4):e36727. doi: 10.5812/ijem.36727. PMID: 28123436; PMCID: PMC5236497.
[53]
Austin GK, Struble SL, Quatela VC. Evaluating the effectiveness and safety of radiofrequency for face and neck rejuvenation: A systematic review. Lasers Surg Med. 2022 Jan;54(1):27-45. doi: 10.1002/lsm.23506. Epub 2021 Dec 19. PMID: 34923652.
[54]
de Felipe I, Del Cueto SR, Pérez E, Redondo P. Adverse reactions after nonablative radiofrequency: follow-up of 290 patients. J Cosmet Dermatol. 2007 Sep;6(3):163-6. doi: 10.1111/j.1473-2165.2007.00322.x. PMID: 17760693.
[55]
- Kang, M. Kislevitz, C. Wamsley, et al., “Clinical Evaluation of the Safety and Efficacy of a 1060 nm Diode Laser for Non-Invasive Fat Reduction of the Flanks,” Journal of Cosmetic Dermatology22(2023): 3017–3025.
[56]
Gutowski KA, Kang A, Kilmer SL, Batra RS, Vignan N, Kenkel JM. Clinical evaluation of the safety and efficacy of a 1064 nm diode laser, and vacuum assisted pulsed electromagnetic fields and multipolar radio frequency for noninvasive fat reduction of the abdomen and flanks. Lasers Surg Med. 2023; 55: 455–463. https://doi.org/10.1002/lsm.23654
[57]
Nilforoushzadeh MA, Heidari-Kharaji M, Fakhim T, et al. Efficacy of Endolift laser for arm and under abdomen fat reduction. J Cosmet Dermatol. 2023; 22: 2018-2022. doi:10.1111/jocd.15684
[58]
Wanitphakdeedecha R, Evangelista KER, Yan C, Apinuntham C, Techapichetvanich T, Eimpunth S, Lektrakul N, Manuskiatti W. The Efficacy of Noninvasive 1060-Nm Diode Lasers for Submental Lipolysis: A Pilot Study. Clin Cosmet Investig Dermatol. 2022 Dec 19;15:2775-2783. doi: 10.2147/CCID.S382582. PMID: 36569419; PMCID: PMC9788834.
[59]
Moon IJ, Choi JW, Jung CJ, Kim S, Park E, Won CH. Efficacy and safety of a novel combined 1060-nm and 635-nm laser device for non-invasive reduction of abdominal and submental fat. Lasers Med Sci. 2022 Feb;37(1):505-512. doi: 10.1007/s10103-021-03288-z. Epub 2021 Apr 2. PMID: 33797649.
[60]
Piłat, Patrycja, Gabriela Szpila, Michał Stojko, Jakub Nocoń, Joanna Smolarczyk, Karol Żmudka, Martyna Moll, and Michał Hawranek. 2023. "Modern and Non-Invasive Methods of Fat Removal" Medicina 59, no. 8: 1378. https://doi.org/10.3390/medicina59081378
[61]
Alizadeh, Z., Halabchi, F., Bodaghabadi, Z. et al. Non-invasive Body Contouring Technologies: An Updated Narrative Review. Aesth Plast Surg 48, 659–679 (2024). https://doi.org/10.1007/s00266-023-03647-x
[62]
https://www.fda.gov/medical-devices/aesthetic-cosmetic-devices/non-invasive-body-contouring-technologies
[63]
Brown SA, Rohrich RJ, Kenkel J, Young VL, Hoopman J, Coimbra M. Effect of low-level laser therapy on abdominal adipocytes before lipoplasty procedures. Plast Reconstr Surg. 2004 May;113(6):1796-804; discussion 1805-6. doi: 10.1097/01.prs.0000117302.73214.1a. PMID: 15114147.
[64]
Avci P, Nyame TT, Gupta GK, Sadasivam M, Hamblin MR. Low-level laser therapy for fat layer reduction: a comprehensive review. Lasers Surg Med. 2013 Aug;45(6):349-57. doi: 10.1002/lsm.22153. Epub 2013 Jun 7. PMID: 23749426; PMCID: PMC3769994.
[65]
Nestor MS, Zarraga MB, Park H. Effect of 635nm Low-level Laser Therapy on Upper Arm Circumference Reduction: A Double-blind, Randomized, Sham-controlled Trial. J Clin Aesthet Dermatol. 2012 Feb;5(2):42-8. PMID: 22468172; PMCID: PMC3315881.
[66]
McRae E, Boris J. Independent evaluation of low-level laser therapy at 635 nm for non-invasive body contouring of the waist, hips, and thighs. Lasers Surg Med. 2013 Jan;45(1):1-7. doi: 10.1002/lsm.22113. PMID: 23355338.
[67]
Thornfeldt CR, Thaxton PM, Hornfeldt CS. A Six-week Low-level Laser Therapy Protocol is Effective for Reducing Waist, Hip, Thigh, and Upper Abdomen Circumference. J Clin Aesthet Dermatol. 2016 Jun;9(6):31-5. Epub 2016 Jun 1. PMID: 27386049; PMCID: PMC4928454.
[68]
Croghan, I.T., Hurt, R.T., Schroeder, D.R. et al. Low-level laser therapy for weight reduction: a randomized pilot study. Lasers Med Sci 35, 663–675 (2020). https://doi.org/10.1007/s10103-019-02867-5
[69]
Wollina U, Wetzker R, Abdel-Naser MB, Kruglikov IL. Role of adipose tissue in facial aging. Clin Interv Aging. 2017 Dec 6;12:2069-2076. doi: 10.2147/CIA.S151599. PMID: 29255352; PMCID: PMC5723114.
[70]
Cotter JD, Taylor NA. The distribution of cutaneous sudomotor and alliesthesial thermosensitivity in mildly heat-stressed humans: an open-loop approach. J Physiol. 2005 May 15;565(Pt 1):335-45. doi: 10.1113/jphysiol.2004.081562. Epub 2005 Mar 10. PMID: 15760945; PMCID: PMC1464483.
[71]
Aquino AE Jr, Sene-Fiorese M, Paolillo FR, Duarte FO, Oishi JC, Pena AA Jr, Duarte AC, Hamblin MR, Bagnato VS, Parizotto NA. Low-level laser therapy (LLLT) combined with swimming training improved the lipid profile in rats fed with high-fat diet. Lasers Med Sci. 2013 Sep;28(5):1271-80. doi: 10.1007/s10103-012-1223-z. Epub 2012 Nov 14. PMID: 23151893; PMCID: PMC3594357.
[72]
Jankowski M, Gawrych M, Adamska U, Ciescinski J, Serafin Z, Czajkowski R. Low-level laser therapy (LLLT) does not reduce subcutaneous adipose tissue by local adipocyte injury but rather by modulation of systemic lipid metabolism. Lasers Med Sci. 2017 Feb;32(2):475-479. doi: 10.1007/s10103-016-2021-9. Epub 2016 Jul 6. PMID: 27384041; PMCID: PMC5288437.
[73]
Duarte FO, Sene-Fiorese M, de Aquino Junior AE, da Silveira Campos RM, Masquio DC, Tock L, Garcia de Oliveira Duarte AC, Dâmaso AR, Bagnato VS, Parizotto NA. Can low-level laser therapy (LLLT) associated with an aerobic plus resistance training change the cardiometabolic risk in obese women? A placebo-controlled clinical trial. J Photochem Photobiol B. 2015 Dec;153:103-10. doi: 10.1016/j.jphotobiol.2015.08.026. Epub 2015 Sep 2. PMID: 26398817.
[74]
da Silveira Campos RM, Dâmaso AR, Masquio DC, Aquino AE Jr, Sene-Fiorese M, Duarte FO, Tock L, Parizotto NA, Bagnato VS. Low-level laser therapy (LLLT) associated with aerobic plus resistance training to improve inflammatory biomarkers in obese adults. Lasers Med Sci. 2015 Jul;30(5):1553-63. doi: 10.1007/s10103-015-1759-9. Epub 2015 May 10. PMID: 25958170.
[75]
Paolillo FR, Borghi-Silva A, Parizotto NA, Kurachi C, Bagnato VS. New treatment of cellulite with infrared-LED illumination applied during high-intensity treadmill training. J Cosmet Laser Ther. 2011 Aug;13(4):166-71. doi: 10.3109/14764172.2011.594065. PMID: 21740089.
[76]
Paolillo FR, Milan JC, Aniceto IV, Barreto SG, Rebelatto JR, Borghi-Silva A, Parizotto NA, Kurachi C, Bagnato VS. Effects of infrared-LED illumination applied during high-intensity treadmill training in postmenopausal women. Photomed Laser Surg. 2011 Sep;29(9):639-45. doi: 10.1089/pho.2010.2961. Epub 2011 Jul 12. PMID: 21749263.
[77]
Ferraresi C, Bertucci D, Schiavinato J, Reiff R, Araújo A, Panepucci R, Matheucci E Jr, Cunha AF, Arakelian VM, Hamblin MR, Parizotto N, Bagnato V. Effects of Light-Emitting Diode Therapy on Muscle Hypertrophy, Gene Expression, Performance, Damage, and Delayed-Onset Muscle Soreness: Case-control Study with a Pair of Identical Twins. Am J Phys Med Rehabil. 2016 Oct;95(10):746-57. doi: 10.1097/PHM.0000000000000490. PMID: 27088469; PMCID: PMC5026559.
[78]
Zagatto AM, de Paula Ramos S, Nakamura FY, de Lira FS, Lopes-Martins RÁ, de Paiva Carvalho RL. Effects of low-level laser therapy on performance, inflammatory markers, and muscle damage in young water polo athletes: a double-blind, randomized, placebo-controlled study. Lasers Med Sci. 2016 Apr;31(3):511-21. doi: 10.1007/s10103-016-1875-1. Epub 2016 Feb 12. PMID: 26873498.
[79]
Ailioaie LM, Litscher G. Photobiomodulation and Sports: Results of a Narrative Review. Life (Basel). 2021 Dec 3;11(12):1339. doi: 10.3390/life11121339. PMID: 34947870; PMCID: PMC8706093.
[80]
Zhao J, Tian Y, Nie J, Xu J, Liu D. Red light and the sleep quality and endurance performance of Chinese female basketball players. J Athl Train. 2012 Nov-Dec;47(6):673-8. doi: 10.4085/1062-6050-47.6.08. PMID: 23182016; PMCID: PMC3499892.
[81]
Rentz, Lauren E., Randy W. Bryner, Jad Ramadan, Ali Rezai, and Scott M. Galster. 2022. "Full-Body Photobiomodulation Therapy Is Associated with Reduced Sleep Durations and Augmented Cardiorespiratory Indicators of Recovery" Sports 10, no. 8: 119. https://doi.org/10.3390/sports10080119
[82]
Magalhães FC, Ferraresi C. Photobiomodulation Therapy on the Treatment of Insulin Resistance: A Narrative Review. Photobiomodul Photomed Laser Surg. 2022 Sep;40(9):597-603. doi: 10.1089/photob.2022.0031. Epub 2022 Aug 30. PMID: 36040371.
[83]
Powner MB, Jeffery G. Light stimulation of mitochondria reduces blood glucose levels. J Biophotonics. 2024 May;17(5):e202300521. doi: 10.1002/jbio.202300521. Epub 2024 Feb 20. PMID: 38378043.
[84]
Al-Atif H. Collagen Supplements for Aging and Wrinkles: A Paradigm Shift in the Fields of Dermatology and Cosmetics. Dermatol Pract Concept. 2022 Jan 1;12(1):e2022018. doi: 10.5826/dpc.1201a18. PMID: 35223163; PMCID: PMC8824545.
[85]
Eskandari SE, Samadi A, Kardeh S, Dowlati Y, Yazdi HA, Firooz A. Photobiomodulation Therapy for Improvement of Body Contour: A Retrospective Study on Middle Eastern Participants. Iran J Public Health. 2024 Aug;53(8):1858-1863. doi: 10.18502/ijph.v53i8.16291. PMID: 39415875; PMCID: PMC11475179.
]]>












































































































































{kind=link}
{kind=link}