
How Far Away to be from Red Light Therapy Panels Part 3: Cold LED Light Therapy
The days of the 6 inches distance "gold standard" from red light therapy panels are long gone.
The ideal distance from a device is where the user will receive the proper amount of intensity. There was never anything special about being 6 inches away to begin with.
After all, we are approximately 93 million miles away from the ultimate red light therapy emitter, the sun. So the distance has always been arbitrary, finding the correct intensity is key.
The latest generation of "highest intensity" red light therapy panels deliver way too much power for the user to be only 6 inches away, compared to the original panels that came to market in 2016.
Yet most companies have not updated their advertised distances because they are trapped by their own marketing narratives.
Intensities >50mW/cm^2 are well documented to risk overheating the skin, cause deleterious tissue response, or quickly reach the unwanted biphasic dose response. [2]
Many users can subjectively confirm they are feeling radiant heating from their "highest intensity" LED panels. Which they falsely assume is a good thing and a sign that they got "good value" from a LED panel.
With traditional "Low-Level" non-thermal light therapy, we need to consider it as a "cold" light therapy, rather than as seeking to use LED panels as glorified heat lamps.
The optimal intensity range for full-body non-contact LED panels is likely between 10 - 50 mW/cm^2, as that is the range seen in most full-body red light therapy studies and recommended by experts.
So if we want to use true medical grade photobiomodulation properly, which by definition is non-thermal, we need be at the correct distance to get the right benefits and not overdose the skin.
What Distance to Use Modern Red Light Panels?
Lets take an example of two panels.
Our GembaRed OverClocked panels versus the SGROW VIGPRO 1500.
Try to imagine the SGROW VIGPRO 1500 as any of your favorite "highest intensity" brands.
The goal is to find the proper distance to be in the 10-50mW/cm^2 range. However, every panel will be different in terms of the power output, number of LEDs, beam angle optics, etc.
So when we measure the intensity at several different distances away, we get the following diagram.

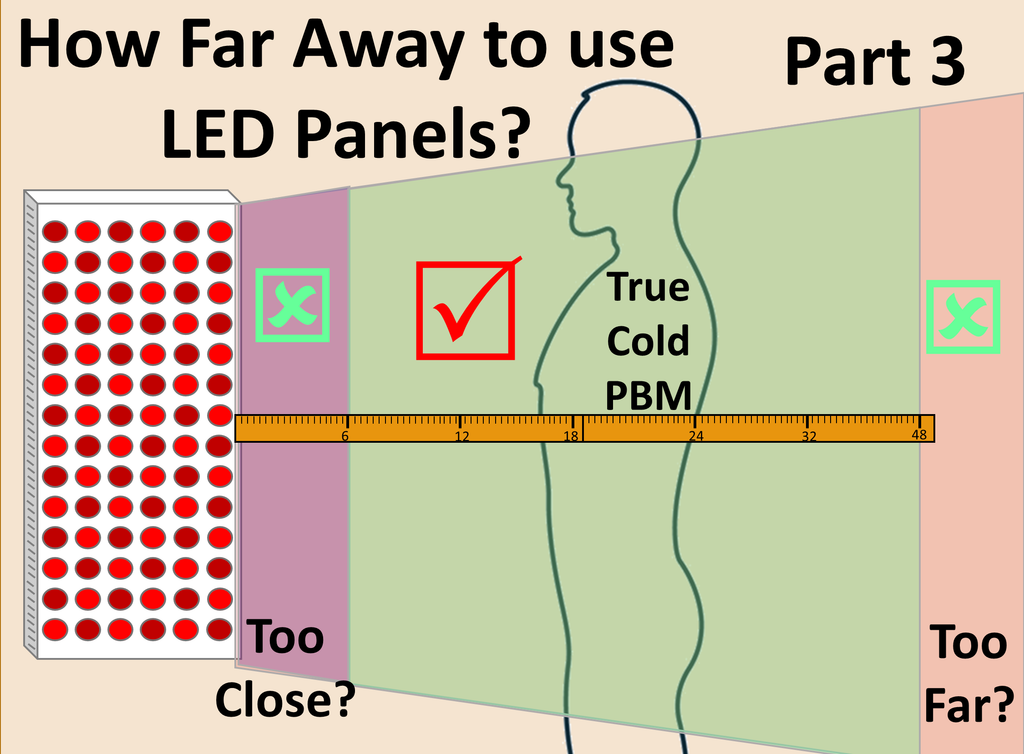
We defined several different "zones" to define the meaning of different distances.
EMF Zone: Most manufacturers recommend being 4-6+ inches away from panels to avoid EMF exposure. This zone usually has many intensity hotspots, poor light uniformity, and poor blending of wavelengths. So even if you aren't concerned with EMFs, it is still ill-advised to use this type of full body red light therapy panels closer than 6 inches away.
Heat Zone: This is a new zone in the advent of the "highest intensity" panel trend. Intensities >50mW/cm^2 can lead to unwanted tissue heating, biphasic dose response, and deleterious effects. So unless you want to use a red light therapy panel as a glorified heat lamp, then you want to increase the distance away until you don't feel any heat.
Ideal PBM Zone: In the range of intensities roughly between 10-50mW/cm^2 is the ideal zone for non-contact non-thermal photobiomodulation (red light therapy) with large LED panels.
Ambient Lighting Zone: At some distance away when intensity is much lower than 10mW/cm^2, or usually even less than 1mW/cm^2 - we don't expect any true photobiomodulation effects. So at great distances away, there is no red light therapy effects, but leaving the light on might be pleasant as a general room light for ambiance.
Both panels certainly deliver sufficient intensities as long as the user is the proper distance away. For the GembaRed Overclocked, which represents first-generation reasonably powered panels, this ideal range is between 6 inches to 48 inches.
For the SGROW VIG1500 and many other "highest intensity" panels on the market, the minimum distance is now 18-24 inches away to avoid the heating zone. So we just shift the effective PBM zone further away to 18 to 60 inches.
No longer is it advisable to be only 6 inches away for such high powered devices.
You Can Never Overdose Red Light Therapy?
Red Light Therapy is often considered to be extremely safe. Experts like Dr. Hamblin will often note a fun-fact that 1 hour of full-body exposure to sunlight (at the equator) is nearly 1 Million Joules of energy.
He says the Red & NIR compenent would not cause harm, but is much more than is needed. He generally uses thise example to explain the extreme safety of the much lower doses used in clinical trials that are effective. Not to actually endorse such high doses.
In another interview he states 10-20mW/cm^2 is "high" for full-body irradiation, and even at 10mW/cm^2 for 10 minutes is about 120,000 Joules of energy. Which is an effective dose, about one tenth of laying in sunlight for an hour at the equator.
However, there is a theory that red light therapy is indeed difficult to overdose, since as the light penetrates the layers of the skin at least one layer is getting the perfect dose.

Although we don't know of any true published literature confirming this theory, it may help explain the wide ranges of effective intensities from 10-50mW/cm^2 and doses from 4 - 60J/cm^2 for a variety of ailements.
However, it is not to imply that extremely excessive intensities or doses are a good idea. Since damaging the skin would create new inflammatory responses that would counteract the benefits we are seeking.

Similarly it is often difficult to "overdose" on drinking water. However, occasionally people can override their logic and die from consuming too much water. We don't want people to override their logic to think that an infinite amount of intensity from red light therapy is fine.
LED Panels as Glorified Heat Lamps
If you are feeling heat from a non-contact LED red light therapy panel, then you are using it as a glorified heat lamp. Since the literal definition of photobiomodulation is clearly defined as a non-thermal interaction of light and biology.
A peer-reviewed article talks about the importance of the definition of PBM:
"The use of this term is key, as it distinguishes photobiomodulation therapy, which is nonthermal, from the popular use of light-based devices for simple heating of tissues as can be accomplished using near-infrared (NIR) lamps, or other applications of light energy that rely on thermal effects for all or part of their mechanism of action. This fact will likely also have significant impact on safety and regulation of commercial products specifically marketed for this use." [1]
Notice the end of the quote is the "significant impact on safety and regulation of commercial products" - which means even LED Panels must abide by this definition of being non-thermal, otherwise they are no longer qualified to call themselves photobiomodulation.
Many studies go through great lengths to monitor skin temperature that it does not increase in clinical trials. As they know it can alter the benefits or lead to detrimental responses.
"LLLT, phototherapy or photobiomodulation refers to the use of photons at a non-thermal irradiance to alter biological activity."[11]
Notice this quote specifically says the irradiance (intensity) needs to be non-thermal. Intensity is the rate of energy delivery and if it is too high then our skin cannot regulate the temperature properly.
Here are a few quotes and peer-reviewed examples to emphasize the importance of not using LED Panels as heat lamps.
Extra Intensity is Heat:
"The photon intensity i.e., irradiance (W/m^2 or spectral irradiance), must be adequate. Using higher intensity, the photon energy will be transformed to excessive heat in the target tissue" [3]
This quote is particularly important because we learn that "higher intensity" does not contribute to PBM benefits, it just gets transformed into heat.
According to this quote, the intensity must be "adequate". Which is a very neutral way of presenting the facts that we don't need too much or too little.
Heating Causes Skin Damage and Biphasic Response:
"Lower irradiance (<50mW/cm2) is less likely to induce skin hyperthermia leading to potential deleterious effects." [2]
"Some studies have shown that there is an increase in collagen degradation and ROS generation with a relatively small increase in temperature." [2]
The excessive ROS which would lead to the unwanted biphasic dose response much quicker, and even "relatively small" temperature increases from high intensity heating can cause this problem.
Mild Heating Hinders Collagen Production:
"Papillary dermis temperature was thus monitored in our clinical study throughout LED exposure to ensure that skin temperature was kept normal in order not to hinder photobiochemical reactions associated with collagen metabolism." [5]
This is key to consider especially for skincare trials to not elevate skin temperature significantly to not alter collagen mechanisms.
Cool Skin Means Better Penetration:
Several studies have indicated that keeping the skin cool will lead to better tissue optics and penetration.[2][6][7]
So if we want to optimize penetration, then we paradoxically don't want too much intensity that would cause dramatic heating.
One study that used cryotherapy before treatment found a 27.5% increase in penetration. [2][7]
Cooling Skin Increases Transparency (penetration of light):
Another study clearly modeled this effect:
"the calculated light penetration depth (d) increased as temperature was lowered, indicating cooling-induced transparency of human skin."[8]
So if people want to optimize photon penetration, then we need to consider intensities and methods that keep the skin cool during treatment.
It is counterintuitive that some "experts" have stated you need very high intensity to optimize penetration, yet too much intensity that causes heating will hinder penetration.
Superficial Absorption Increases with Temperature
Many falsely assume that skin optics stay constant with temperature. It does not, and several studies have investigated this fact.
One study found an increase of absorption coefficient of 10.1% per degree Celcius raise in tissue temperature.[9] This would directly correlate to a loss of penetration, as well as create a snowball effect of even more superficial heating.
The same study states the following:
"On the other hand, tissue temperature during LLLT should be maintained below 40 °C, for thermal damage of tissue can occur as the temperature rises above 40 °C" [9]
So for "true" photobiomodulation therapy, the skin temperature should remain below 40°C (104°F) during treatment. If normal skin temperature is between 33-37°C (92-99°F), then it is allowable for a small temperature increase of 3-7°C (5-12°F).
However, for every degree increase there could be a loss of penetration due to increase absorption coefficent. As well as increased ROS as noted in the previous studies. [2]
PBM First, Heating Second
From a textbook on LLLT, the authors tell us this:
"If heat is used in combination with laser therapy, the laser treatment should come first. Heat will increase blood flow in the tissue, thus increasing the absorption of the light in blood. The opposite then applies to cryogenic therapy."[13]
So the authors are summarizing what we already learned, that heating increases absorption which decreases penetration to the target tissue. So to do light therapy before heat therapies (and not combine them like a full-spectrum sauna).
Not Exceed 1°C and High Intensity Laser Therapy (HILT) vs LLLT
One study comparing the differences between LLLT (Low-Level-Laser-Therapy) and HILT (High-Intensity-Laser-Therapy) noted that LLLT is almost always a temperature change of less than 1°C. They also show that LLLT lasers are less than 500mW and HILT lasers are greater than 500mW. [12]
In that regard perhaps we should draw a line for large LED light therapy that any panels above >100mW/cm^2 at treatment distance should certainly be considered more of "High Intensity LED Therapy" and no longer true "Low-Level-Light-Therapy".
Twice the Intensity Means Different Benefits:
"if the power doubled and the time is halved then the same energy is delivered but a different biological response is often observed." [4]
We get a different biological effect if we double the intensity but decrease the exposure time in half. This mathematically works for Joules (energy), but the studies often discourage this concept as it does not work as predicted. The human body is not a linear math equation.
So companies that claimed to be "twice the intensity of Joovv" never actually proved that was more effective or superior for therapy. They just were using a false "value" proposition that was never based in science.
Cold LED Light Therapy
You may be familiar with the term "cold laser" in the LLLT/PBM clinics.
Technically these lasers are not truly "cold", but they mean to imply that these lasers are low enough power not to produce heat. The name is an important reminder that Photobiomodulation uses low-level non-thermal lasers.
Here is one direct quote:
"This process is referred to as ‘low-level’ because the energy or power densities employed are low compared to other forms of laser therapy such as ablation, cutting, and thermally coagulating tissue." [11]
So we know lasers can be heating devices which is why the high-powered ones are excluded from LLLT/PBM. And again, the energy and power density (another term for intensity) is the key criteria to define a heating response.
It was assumed that LEDs could not get powerful enough to cause too much of a heating response. But as most technologies develop on an exponential curve, we have already witnessed the "heating" LED panels on the market.
Perhaps now we should coin a term for "Cold LED therapy" to distinguish true medical grade photobiomodulation panels. The "highest-intensity" heating LED panels will now be excluded from photobiomodulation, the same way high-powered lasers are excluded from this therapy category.
Few will remember the Heliotherapy clinics and Open-Air Hospitals that were opened in the early 1900's that preferentially were located in "cool" mountain air. [10]
One direct quote from "the Sun Doctor" Auguste Rollier who opened one of the first clinics in Leysin, Switzerland in 1903:
"The intense heat of the sun is tempered and rendered wonderfully bracing by the action of the dry, cold air on the whole surface of the body."[10]

So even before Endre Mester discovered LLLT with his cold lasers in the 1960's, the Heliotherapy doctors in the 1900's already knew the importance of "cold" light therapy.
Conclusions
Having the "highest intensity" LED Red Light Therapy panels didn't add more value or effectiveness. They only increased the distance the user needs to be to be in the appropriate PBM Intensity range.
Yet, without updating their advertised distances away from 6 inches, higher intensity panels may indeed be less effective if used improperly.
If users are seeking heat devices, they could save a lot of money and just buy an incandescent heat lamp, rather than an expensive overpowered LED Panel.
Otherwise we should keep in mind that we want "cold" light therapy to be true medical-grade photobiomodulation.
The "first generation" red light therapy panels and reasonably powered red light therapy panels can indeed be used properly at 6 inches away up to about 48 inches away to stay in the correct intensity range.
The "latest generation" high powered LED panels may require to be much further away, with a minimum distance of 18 or 24 inches away (2 feet!), and perhaps the effective distance is also extended to 60+ inches away and still get benefits.
While "being further away" may seem attractive, there are certainly scenarios where there is limited space for a user to be able to stand 2+ feet away from a panel. Especially for clinics that want to position panels on both sides of the users, it would take up a lot more space as shown below.

Having to be "far away" from a panel can take up a large footprint in a small apartment, clinic, or closet - especially trying to position multiple panels for each side of the body.
Yet the marketing narrative has not been updated by most major brands, and many consumers are enjoying the instant gratification of using LED panels as glorified heat lamps. Occasionally with detrimental effects of skin pigmentation or eye complaints.
Children and Pets may not be able to comprehend that they need to be 2 feet away from red light panels for safety, even if brands start updating their recommended distances.
The technology is rapidly evolving and growing more powerful, yet the marketing strategies also need to evolve to abandon the "6 inches" standard in favor of advertising distances that deliver the right intensity for safety and effectiveness based on the actual clinical science.
In the absence of honest intensity advertising or updated recommendations to increase the distance, our original recommendation from the first part of this series stands as prophetic and timeless.
Just keep increasing your distance away from the panel until you don't feel any heat anymore. That's the best "science" you can get while using the "top" brands that don't share accurate intensity data.
End
Read Part 1 of this series to learn about how being 6 inches away was not supported by the science, and was a byproduct of faulty product design and clever marketing.
Read Part 2 of this series to learn the optimal ways to use non-contact red light therapy, assuming one is aware of the differences between the two main methods of red light therapy treatments.
[1]
Kim, S., Jeong, S. Effects of temperature-dependent optical properties on the fluence rate and temperature of biological tissue during low-level laser therapy. Lasers Med Sci 29, 637–644 (2014). https://doi.org/10.1007/s10103-013-1376-4
https://link.springer.com/article/10.1007/s10103-013-1376-4
[7]