
Engineer's Guide to Selecting Wavelengths for Photobiomodulation / Red Light Therapy
When shopping for red light therapy we commonly talk about wavelengths of light! This may be important to help understand the efficacy and application of certain devices for various benefits. Using the right wavelengths or combinations of wavelengths could mean the difference between a beneficial effect, or no effect.
However, as a company run by an engineer, we aren't going to pretend to be internet doctors selecting wavelengths for their health benefits. Nor do we have time to read through all of the 4000+ publications on the topic and cherry-pick the most marketable articles to reference. Like a laser, we find a straight path to the best wavelengths. This is how.
Customer Experience:
The #1 criteria for lean engineering design is to consider your customer needs and interests. We see that most popular designs incorporate multiple wavelengths of red light, preferably a combination of visible red and invisible near-infrared. So the goal is to find multiple wavelengths that we can incorporate logically into a product.
The Optical Window:
The general consensus is that light between 600nm to 1000nm is ideal for red light therapy or PBM. No reference here as this is reiterated in the introduction or background section of most PBM articles.

True to the word, shorter than 600nm is no longer red light therapy, as it is yellow and has shallow penetration. As we approach the longer invisible near-infrared studies agree there is better penetration, however too long of wavelengths particularly after 1000+ start to get absorbed by the water in the body as heat. (1)

Within this window studies observe the best penetration due to scattering properties of skin, tissues, and blood. The mechanism of action is considered to be modulation of Cytochrome C Oxidase in the mitochondria which activates many downstream benefits such as increased ATP production and release of Nitric Oxide. Utilizing multiple wavelengths of red and near-infrared seems to have indication of modulating different states of the Cytochrome C Oxidase in the respiratory chain.
Commercial Availability:
Knowing the sun is a continuous spectrum of all the wavelengths including the range of PBM of 600nm-1000nm, you would like to think that doctors, scientists, and manufacturers of PBM devices are selecting the precise wavelengths from the spectrum for optimal benefits.
The sad truth is that we are limited by the technology and commercial availability of emitters. A laser or LED uses a semiconductor diode to generate the wavelengths, the type of materials used to make the diode determines what wavelength it will emit. (2) As such we currently have limited wavelengths available to us based on the materials that have been developed so far. This would explain why we see the same wavelengths studied over and over again, because that is what is available (and affordable).
Knowing what wavelengths are available is the first step to selecting the right ones.
Down-select The Most Popular Wavelengths:
Here is the fun part. Download a copy of the LLLT google document complied by Vladimir Heiskanen. (3)
www.bitly.com/PBM-database
Open the spreadsheet in Microsoft Excel. Highlight the column for Wavelengths, and Search (ctrl+f) each of the commonly used wavelengths with the "Find All" feature, and read the # of hits that it gets.
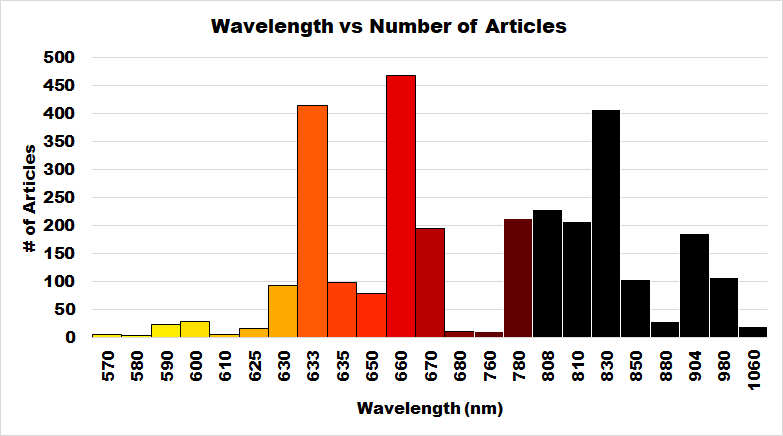
This is the result from a download of the spreadsheet on 1/18/2019 and 4085 studies.

An engineer with more free time on his hands might even filter out or delete out the studies that have had neutral results, but for now this is a good swag.
We see here overwhelmingly that 633nm, 660nm, and 830nm wavelengths are the most prevalent in studies, each with over 400 articles! The close second would be 670nm, and low 800nm wavelengths with around 200 articles each.
Does this mean that these are the best wavelengths to use for PBM? Not necessarily, it just means we have a lot of data around them. Being data-driven, that is what we like.
Know the spread:
We understand that our LEDs can have up to +/- 20nm spread of output of wavelengths (unlike a laser which emits a near-single wavelength) helps us further select the most ideal wavelengths.
For example, a 630nm LED will easily cover 633nm and 635nm, so you get the benefits of those wavelengths as well.
Then obviously a 660nm wavelength will also cover nearby 650nm, 670nm.
When we debated selecting between 830nm or 810nm, both of which are great wavelengths. We decided not to do 810nm, because too much of the spectrum will dip into the 700's, which is generally a less interesting region for PBM. By choosing 830nm, we get the benefits of the low-800's with optimal efficiency.
Similar for our 850nm wavelength, that overlaps much of the mid-800's region. The truth is that 850nm is generally lower cost than 830nm LEDs, so that is why it is more prevalent in commercial PBM products, and why we can offer our GembaRed Groove at a lower price than the GembaRed Rex.
Put it all together:
So there we have it. The first honest and practical way of analysis of wavelengths with zero claims of benefits.
Future Work:
We hope that Vladimir & team will continue to find time to continually update his spreadsheet, as the rate of published studies is rapidly increasing over time. We also hope that parameters such as dose, intensity, cumulative dose, treated area, and outcome become easily searchable and index-able in the spreadsheet. This would allow for multivariable analysis to be performed to help design optimal treatments and protocols.
References:
(1)
"The Optics of Human Skin"
https://www.sciencedirect.com/science/article/pii/S0022202X15461251
(2)
https://en.wikipedia.org/wiki/Laser_diode
(3)
Low Level Laser Therapy (LLLT) spreadsheet
www.bitly.com/PBM-database