
How Deep Does Red and Near-Infrared Light Penetrate into the Body? Marketing vs. Science
How deep does red light therapy really penetrate through the skin? Can it really reach and directly affect our muscle tissue or brain? Do we even need that much penetration to know it is effective?
One of the main properties of Red and Near-Infrared (NIR) light (between 600nm to 900nm) is its unique ability to penetrate through the skin further than any other wavelengths on the “light” spectrum (from UV to Far-Infrared).
The common statement is that Red wavelengths (600nm-700nm) offers less depth penetration than NIR (700-900nm).
However, describing Red as “less penetration” is only a relative term.
How much difference is there between Red and NIR? How deep does Red and NIR actually reach? That’s what we will dig through the research to find out.
And of course we need to answer the burning questions if Red or NIR actually can penetrate to the Brain, Gut, Muscle, or other target tissues that are deeper in the body. Since our simplistic view is that we may need to directly stimulate those areas with light to illicit a beneficial response. Could we be wrong in that assumption too?
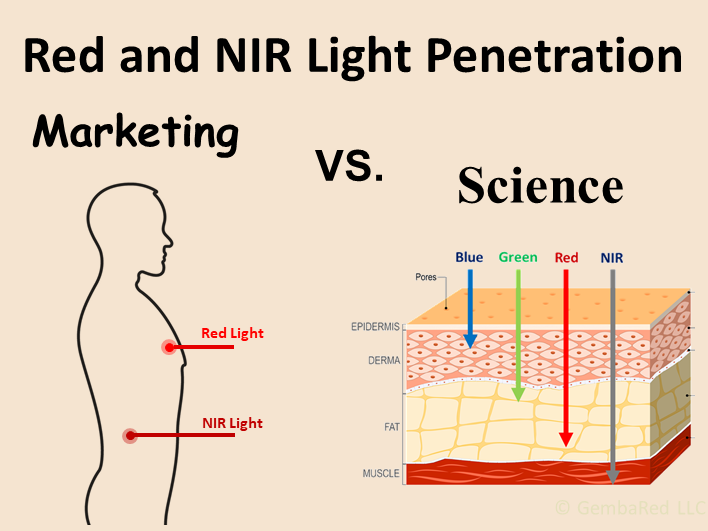
Marketing Oversimplification:
Based on the oversimplification that Red has more superficial penetration and NIR having deeper penetration, this leads to some myths about the applications and benefits of these wavelengths.
Superficial: A fancy way of saying “lacking in depth” or only on the surface. https://www.merriam-webster.com/dictionary/superficial
So even using this term gives an inferior connotation to Red light compared to NIR.
In fact, some of these myths are not only imaginary, but have been falsely illustrated over the years.

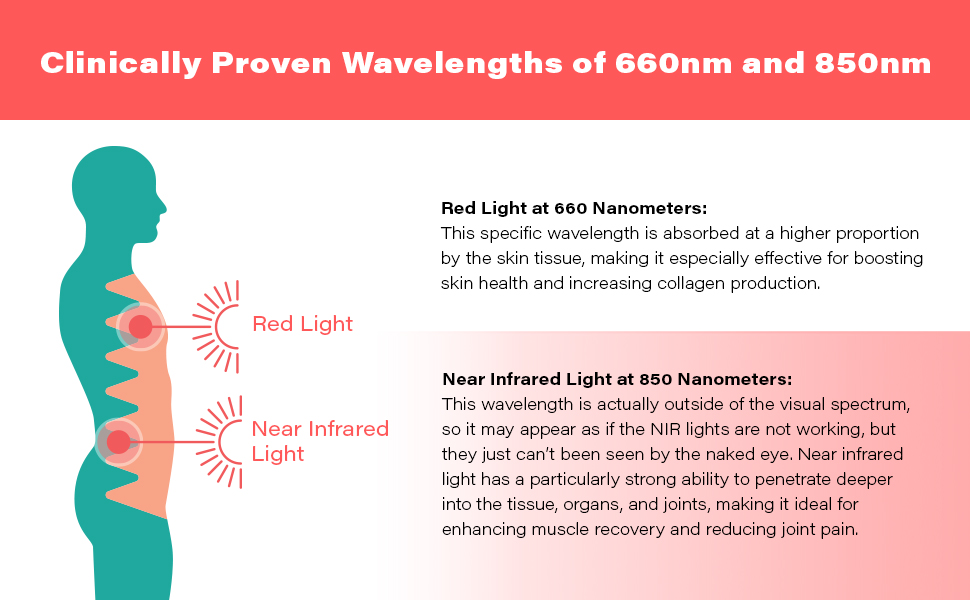
This diagram is Not To Scale, and similar diagrams have been used by Joovv and now other companies like Hooga and Bestqool. These diagrams give a drastically false impression of the relative depth penetration of these wavelengths, as well as the seemingly tremendous penetration of NIR!
{kind=link}
{kind=link}
And these kinds of marketing fallacies also make consumers think that NIR wavelengths are ONLY good for deep penetration, and that Red is ONLY good for skin treatment. Which is a disturbing fallacy and there is a lot of overlap of benefits between both Red and NIR.
Scientific Diagrams of Penetration:
Like most things in understanding the science of Photobiomodulation, the first thing we need to do is empty our minds of anything that other red light panel companies have claimed, and get our facts straight from PubMed. It seems lately the only thing worth reading on competing blogs is based on references and topics that they find on our blog.
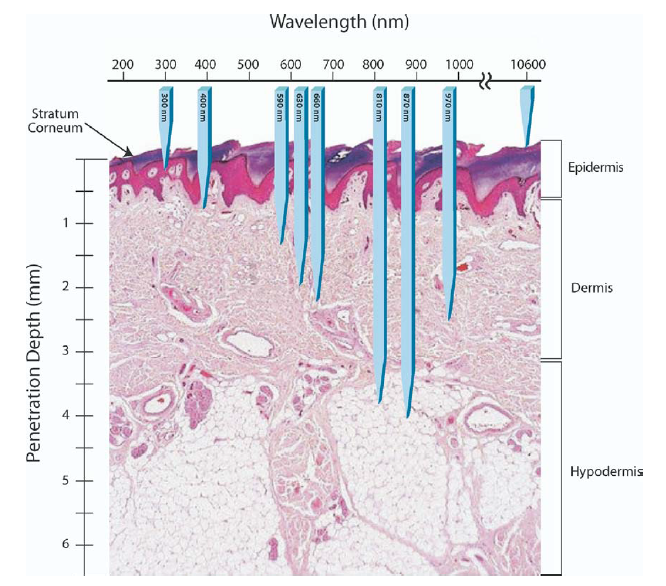
Here is a diagram that is similar to what we find in actual studies:

Now we see that this diagram zooms into the layers of the skin, and the scale is perhaps only 5 millimeters, not an entire body!
You can find similar diagrams that are actually to scale in these studies:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5653719/
https://api.intechopen.com/media/chapter/48345/media/image5.png
{kind=link}
We will discuss this more later, but look closely at the diagrams, we start to see that there is only a subtle difference between Red and Near-Infrared. It is only a difference of a couple millimeters resulting in a 10-30% difference between Red and NIR wavelengths based on the scale in those diagrams.
What is the definition of Penetration in Red Light Therapy?
Before we go any further, what is the definition of penetration for red light therapy? In science and engineering, it is important to DEFINE terms like this so we can all “speak the same language” and make sure we are standardizing our study approach.
Obviously we don’t just want a trace amount of photons reaching a certain depth, we want a meaningful and therapeutic amount of power reaching the target tissue.

Lets say that we use an 810nm wavelength at 100mW/cm^2. Only 10% of that intensity reaches 1mm depth. So that means 10mW/cm^2 reaches the 1mm depth.
And only 1% of that intensity reaches 2mm depth, meaning only 1mW/cm^2 reaches 2mm. So most people might say that at the 2mm depth is not particularly an effective intensity that reaches there. This is a real example taken from this study.
The Optical Window for Skin Penetration:
We are primarily focused on what we might call “transdermal” penetration of red light therapy, meaning "through the skin". Other times studies refer to "transcranial" photobiomodulation, which is through both the skin and skull. Our skin is the first most obvious barrier to limit penetration, since it must protect us from excessive sunlight, heat, and cold.
Since most consumer products for home-use are naturally transdermal because they are aimed at the skin. Then that is what we are looking at for this blog.
The reason that penetration is mostly “wavelength dependent” is due to the optics of the skin. We discussed in a previous blog how the “optical window” is where there is the least absorption by melanin, hemoglobin, and water between 600nm to 900nm. So, of course, there is acknowledgement that the constituents of our tissues are what really controls the wavelength penetration.

Most studies seem to agree that around 810nm (sometimes 808nm if it’s a laser study) offers the best penetration since that is the lowest intersection point of absorption factors. It has also been confirmed in some comparison studies between wavelengths.
Penetration Depth Graph:
In one study, researchers were able to mathematically calculate the penetration of light from 200nm to 1000nm through the skin.[20] This was through complex formulas of understanding tissue optics for several layers of skin, including the absorption factors we mentioned above, along with scattering coefficients in the skin.
The following graph gives us a great visualization of the "optical window" range that we expect from 600nm to 900nm:

https://onlinelibrary.wiley.com/doi/10.1111/php.13550
The different lines correspond to the percentage of intensity that reaches a corresponding depth.
So we see that only 1% of intensity reaches about 5mm deep from the range of 660nm to 880nm. The majority of the intensity (50%) only ever reaches up to 1 to 1.3mm deep - even in this ideal optical window for penetration.[20]
Penetration Comparisons at Different Wavelengths:
So what do studies say as they compare the penetration of different wavelengths?
A review article by Dr. Hamblin states that red wavelengths (600-700nm) penetrates up to 1mm and NIR (780-980nm) penetrates to 2mm with 63% of the intensity reaching those depths. [1] That doesn't seem like much much penetration at all, although that percentage transmission is quite high.
A study using mathematical modelling of skin optics details that 633nm penetrates to 1.8mm, 660nm to 2.0mm, 850nm to 2.4mm, and 900nm to 2.5nm. [2] Again, not nearly as much as we expected!
Another study using mathematical modelling of penetration profiles shows the Red at 650nm reaching about 4.5mm and the NIR at 750nm reaching past 5mm. [3]
A study using cadaver heads with the scalp/skull/brain in tact looked at the penetration profiles through those tissues. They found that the Red wavelength of 660nm reached 21mm and the 808nm reached 40mm. [4] This is good news for some people wanting to make sure it reaches the brain!
Finally, another study looking at penetration differences noted only a 10% difference in light transmission when comparing wavelengths ranging from 630nm to 905nm. [5]
Similar to the range of doses used in studies, there is a wide range of penetration results from different studies. The difference in penetration between Red and NIR might only be 10% according to some studies, and according to other studies Near-Infrared offers DOUBLE the tissue penetration compared to Red.
How Intensity Affects Penetration:
Like most things in Red Light Therapy, it is the intensity that is critically important. It is a shame that most red light panel companies measure it wrong or are purposely misleading about intensity.
From the first example earlier with the 810nm only having 1% of the power reaching 2mm deep. What if we really need 10mW/cm^2 to reach 2mm deep? Could we just use a 1,000mW/cm^2 intensity at the surface? Probably, but that is a lot of intensity to load onto the skin just to reach a deeper target.
One study looked at increasing intensity and resultant depth penetration. They used a 660nm light and increased intensity to observe the penetration. They found that 100mW/cm^2 penetrates to tissue less than 50mm deep. They found to go deeper than 50mm required a “disproportionate” increase in intensity. [6] Note that even 50mm penetration is quite impressive for 660nm red light!
A review article estimates that a 1 Watt NIR laser (760-850nm) delivering 5,000 mW/cm^2 (yes, 5 thousand mW/cm^2) on the skin surface can deliver 5mW/cm^2 at 5 cm deep. [20]
Another study found that they needed a 15 Watt 810nm laser to penetrate 2.9% of the power 3cm through the skin and skull and into the brain. [7] That is a disproportionate intensity indeed!
Another study commented on the excessive intensity that would be required to reach a significant depth into the brain.
“These energy density dosages would be difficult to achieve and would likely cause significant and potentially damaging thermal effects.”[8]
We know that too much intensity would lead to overheating of the skin, it may not be safe or practical to attempt to use so much power simply to affect the brain or reach deeper penetration.
Does Pulsing Improve Penetration?
To avoid dramatic tissue heating and damaging the skin caused by increasing the intensity, some studies employ pulsing.
As we discussed in detail in our previous blog, pulsing is a rapid “on” and “off” of the LED or Laser. According to one study:
“The “quench period” (pulse OFF times) reduces tissue heating, thereby allowing the use of potentially much higher peak power densities than those that could be safely used in CW” (CW is continuous wave)[9]
*note, you might notice this scientific definition is very different than the illogical definition of "quench" given on the Ben Greenfield and Joovv blogs*
So indeed, pulsing does potentially enable greater penetration but only when it is combined with higher peak power. Be wary of companies making claims out of context that just pulsing their light will magically increase penetration, they need to vastly increase the peak power too. Which we don’t think they are doing.
In fact, in studies where they do NOT increase the peak power of the pulsed mode, it is clear there is a loss of penetration.
For example, one study on the "Mean Output Power" (MOP) through living dog tissue found that CW (continuous) offered better penetration than PW (Pulsed).
"Regarding the operation mode, the MOP of the CW mode was obviously greater than the PW mode. This result is consistent with a study on the penetration of LILT in anesthetized rabbits. Thus, the CW mode of LILT is recommended for the treatment of deeper organs excluding thermal side effects." [14]
So it was concluded from this study that deeper treatments should be done with Continuous Wave unless heating becomes a problem due to too much intensity.
Which skin heating generally isn't a problem with standard LED panels, so adding pulsing to panels is generally unnecessary, and may even detract from the dosage and penetration.
Skin Contact for Penetration:
Resoundingly when we investigate penetration, many studies mention the importance of skin contact. Otherwise the intensity is lost to reflection and refraction from the skin.
One study states it as such:
And in a previous blog we showed how the skin can reflect away on average about 60% of the light in the Red and NIR range. That is a significant loss of light!

Our illustration of non-contact vs skin contact. A similar diagram with lasers can be found in this study. [17]
Our other blog on how skin contact shows a study measuring the apparent loss of penetration when comparing non-contact to contact treatment.
Another study noted that contact method is 5 times more efficient at transcutaneous penetration than with non-contact treatment. [19]
Taken together, it paints the picture that LED Panels that advise people to be 6+ inches away will have much less penetration than we may have been led to believe.
Red or NIR benefits? Which one to use for particular applications?
Of course we want to see the effects and applications of wavelengths, so lets look at a couple of studies that debunk the typical logic.
Red Wavelengths for The Brain:
One study used 660nm at only 9mW/cm^2 and another study used 627nm at 70mW/cm^2 and both showed positive results to improve brain function. Both studies were applied transcranially, although according to the usual logic most people would scoff and say those wavelengths and intensities would not be applicable for the brain. [11] [12]
The famous “Red Light Bucket Hats” were primarily made with 670nm strip lights and have been reported to be successful for Parkinson’s patients. And red strip lights aren’t particularly high intensity either. So again we have a situation where people might not “believe” they are effective for transcranial applications, yet they debunk the common knowledge.

Some of our customers have constructed the "Cossack" hat from red strip lights and following the instructions on this blog. Can it even be effective with low power Red LEDs?
Red Vs NIR for Muscle Recovery:
One study comparing 660nm versus 830nm for athletic recovery and found no significant difference in benefits between the two wavelengths. They were essentially the same. [13]
Again, for muscle recovery, we might have assumed the 830nm would be superior due to its implied deeper penetration.
NIR Wavelengths for Skin:
A recent review article titled "Near-Infrared Light and Skin: Why Intensity Matters" helps dispel many myths about Near-Infrared wavelengths being detrimental to the skin. They clairfy that most detrimental studies used exessivly high intensity, and intensities greater than or equal to 100mW/cm^2 are associated with photoaging of the skin. Whereas they state intensities in the range of 30mW/cm^2 offers Photorejuvenation for the skin! [15]

There is much more overlap of the benefits and applications of Red and NIR wavelengths than many people think. Red can help the brain, and NIR helps with skin! Especially now that we consider the penetration isn't as different as we thought.
How much penetration do we really need?
So maybe we are somewhat disappointed that Red and NIR doesn't seem to penetrate as deeply as the misleading marketing diagrams showed us. So what?
One study noted this when they measured only 1% penetration through tissue-folds for Red and NIR:
“This suggests that the critical light-tissue interactions for effective PBMT occur in the skin at the capillary level and that effects on deeper structures are secondary, chemically-mediated events." [16]
This implies that there are indirect and “systemic” benefits to red light therapy that are carried deeper into the body by the blood and cellular mechanisms themselves, not by direct influence of the light.
A review of photobiomodulation for brain disorders by Dr. Hamblin had this to say about the apparent lack of penetration of the light into the brain:
“It is in fact very likely that the beneficial effects of PBM on the brain cannot be entirely explained by penetration of photons through the scalp and skull into the brain itself.” [17]
And this quote was in a section regarding systemic benefits of red light therapy for the brain, and postulating that systemic benefits are a more likely explaination than direct light penetration. [17]
This may explain why studies employing lower intensities or red wavelengths for the brain still show positive results.
While we know a lot about how to optimize penetration with the right wavelengths, responsible intensity, skin contact, and maybe pulsing – it might not be necessary to be too distracted on the exact millimeters depth it actually reaches.
Conclusion:
Clearly we see a wide range of data on penetration ranging from 1mm to 50mm for both Red and NIR.
The most repeatable data seems to indicate that both Red and NIR may effectively reach around 2-5mm with reasonable amounts of intensity to deliver a therapeutic response to the tissue. Altough some studies with higher intensities reach 40-50mm with both Red and NIR.
NIR offers somewhere between 10% more to 100% (double) more penetration compared to Red wavelengths depending on the study.
Since penetration also depends on skin contact and intensity, it is even more important for LED panel companies to be honest about intensity and understand the drawbacks of recommending people stand 6 inches away.
While pulsing may allow for more penetration in some contexts to increase intensity and prevent overheating, generally continuous wave is preferred for penetration and dosage. That won't stop Joovv and other copycat brands from adding pulsing features to their panels and making creative new marketing claims.
The good thing is that even despite the false advertising and apparent lack of penetration that pulsing non-contact LED panels really offer, customers of LED panels are still getting great benefits!
Is it the placebo effect? No. It is likely the systemic benefits we discussed earlier.
So we don't neccessarily need to blast our heads with high intensity light just to get a beneficial effect. In fact, that is clearly ill-advised due to the skin damage it could cause. It is important to have patience and trust our body to deliver the secondary effects deeper into the body.
And of course we know that Red wavelengths can benefit the brain, and Near-Infrared wavelengths can benefit the skin! There is hardly any reason to shun any particular wavelength until we get more data. Although Red is still preferred for the skin and NIR is still perferred for deeper penetration, there is still a lot of overlapping benefits of both.
Until we learn more about Red and NIR mechanisms and penetration, we can’t let oversimplifications about Red and NIR steer us in the wrong direction. While even we at GembaRed employ some of these generalizations, digging deeper into the science only reveals how much we don't know yet.
-Andrew
[1]
Optical properties of human skin, subcutaneous and mucous tissues in the wavelength range from 400 to 2000 nm
A N Bashkatov, E A Genina1, V I Kochubey1 and V V Tuchin1
Published 22 July 2005 • 2005 IOP Publishing Ltd
, , Citation A N Bashkatov et al 2005 J. Phys. D: Appl. Phys. 38 2543
[9]
Hashmi JT, Huang YY, Sharma SK, et al. Effect of pulsing in low-level light therapy. Lasers Surg Med. 2010;42(6):450-466. doi:10.1002/lsm.20950
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2933784/
[10]
[11]
Salgado, A.S.I., Zângaro, R.A., Parreira, R.B. et al. The effects of transcranial LED therapy (TCLT) on cerebral blood flow in the elderly women. Lasers Med Sci 30, 339–346 (2015). https://doi.org/10.1007/s10103-014-1669-2
https://link.springer.com/article/10.1007/s10103-014-1669-2
[12]
Kampa N, Jitpean S, Seesupa S, Hoisang S. Penetration depth study of 830 nm low-intensity laser therapy on living dog tissue. Vet World. 2020;13(7):1417-1422. doi:10.14202/vetworld.2020.1417-1422
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7429387/
[15]
Shining light on the head: Photobiomodulation for brain disorders,
BBA Clinical,
Volume 6,
2016,
Pages 113-124,
ISSN 2214-6474,
https://doi.org/10.1016/j.bbacli.2016.09.002.
(https://www.sciencedirect.com/science/article/pii/S2214647416300381)
The Proximal Priority Theory: An Updated Technique in Low Level Laser Therapy with an 830 nm GaAlAs Laser
www.jstage.jst.go.jp/browse/islsm
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3882347/
[19]
https://www.spiedigitallibrary.org/conference-proceedings-of-spie/10861/108610N/What-is-the-prospect-of-transcutaneous-transmission-of-980nm-photobiomodulation/10.1117/12.2506435.short?SSO=1
[20]
Cotler HB, Chow RT, Hamblin MR, Carroll J. The Use of Low Level Laser Therapy (LLLT) For Musculoskeletal Pain. MOJ Orthop Rheumatol. 2015;2(5):00068. doi:10.15406/mojor.2015.02.00068
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4743666/
[21]