

810nm vs 830nm: The Best Wavelengths for Red Light Therapy
What is the best wavelength for Red Light Therapy?
The "optical window" of wavelengths preferred for Red Light Therapy are the Red to Near-Infrared (NIR) range from 600nm to 1100nm.[1]
But which one is the absolute best?
In this blog we will propose that 830nm Near-Infrared is the best wavelength for Red Light Therapy.
It will likely take decades more of research to truly find the best wavelengths for Red Light Therapy, and even then it will be nuanced and based on context.
So, this will be a "thought experiment" and discussion around what we would look for in the best wavelength. Using 830nm as the model that currently seems to have the best evidence supporting it.
What defines the best wavelength? The deepest penetration? The best benefits? The safest? The best systemic effects? The most successful studies? Or that it activates important biological mechanisms? Yes.
What We Learned:
- 850nm is not the best Near-Infrared Wavelength according to the current research.
- The clear best NIR wavelengths are 810nm and 830nm.
- While 810nm may have modestly better penetration than 830nm, this is only achieved with skin contact method. The superiority of 810nm is lost when using non-contact red light therapy therapy (i.e. LED panels at 6+ inches away).
- 830nm shows to have superior systemic mechanisms by being closer to the peak absorption spectrum for Cytochrome C Oxidase.
- 830nm has been shown to be versatile for not only deep penetraton, but also for superficial benefits like skin care, wound healing, eye health, and hair health. As well 830nm having been clinically studied specifically with non-contact LED devices.
- Non-contact devices (i.e. LED panels) will do better with 830nm for its superior systemic mechanisms, and perhaps skin-contact devices should prefer 810nm in cases requiring the deepest penetration.
850nm - The Best Wavelength that Researchers Forgot About:
Even a rudimentary analysis of the database of studies shows that 850nm is not the most popular Near Infrared wavelength for red light therapy.
We should expect to find overwhelming scientific studies and doctors and researchers clearly stating that 850nm is the best. Which is conspicuously absent when you start reading the research.
Lets look at some quotes from peer-reviewed published articles by real researchers and experts.
- The following 2023 review article on using Photobiomodulation for muscle function reviewed 29 studies (narrowed down from thousands) to make this conclusion:
"It is believed that optimal wavelengths are near 810 – 840 nm, since in these regions the surface chromophores have weak absorption, and therefore there is maximum penetration of light into the skin, generating an optimal window of penetration and absorption by organic molecules [38]." [2]
This quote establishes that the range between 810nm to 840nm contains the best wavelengths especially for penetration and absorption mechanisms. Unfortunately, 850nm is excluded from this range and is implied to be less optimal than the wavelengths within this range.
- Another December 2022 review article on Photobiomodulation for eye health makes this statement as part of their literature analysis:
"Red to near-infrared light photons with long wavelengths can directly transfer energy to cytochrome C oxidase, leading to an increase in enzyme activity and energy metabolism, which may play a key role in further inducing PBM. Based on the literature summary above, light wavelengths at 635–680 nm and 810–830 nm are more suitable for inducing PBM to treat retinal diseases." [3]
Again, conspicuously excluding 850nm while highlighting the optimal range of 810-830nm for eye health.
- A 2016 study on wound healing makes this comment about the ideal wavelengths for penetration and mechanisms:
"Both scattering and absorption of light by tissue are highly wavelength-dependent and NIR light around 810–830 nm have been found to have the deepest penetration and homogeneous illumination of the full dermis and part of the hypodermis [12,15]." [4]
- One 2019 review article on transcranial Photobiomodulation (red light therapy on the brain) for depression made this conclusion about the ideal parameters to optimize penetration and effectiveness for brain health.
"Based on the data presented above, using wavelengths in the range of 808–835nm, laser devices, higher power densities, and pulsed parameters will likely increase efficacy." [5]
- A 2018 review article on using Photobiomodulation for Cardiovascular Health and Nitric Oxide production made this statement about the most researched wavelengths from their review:
"The most extensively studied spectrum for PB includes light
in the spectrum of 630–830 nm." [6]
It is disturbing that so many of these quotes don't include 850nm within their range of the most studied wavelengths and/or optimal wavelengths for PBM.
- A 2020 review of LLLT for pain management had this to say in their conclusions of the best wavelengths for pain:
Bjordal et al find that wavelengths of 632 to 660 nm, or infrared lasers with wavelengths of 810 to 830 nm, show anti-inflammatory effects" [7]
They don't directly mention 850nm in the article quoted above, but they note the average wavelength of 846nm was associated with negative outcomes compared to wavelengths closer to 810nm were associated with positive outcomes.
- A 2016 study had this to say about the typical wavelengths used to treat pain:
"For clinical pain relief, the usual wavelengths are in the red range (λ=632.8 and 670 nm) and in the NIR (λ=780; 810 to 830; 904 nm)." [8]
Now this quote purposely skips over 850nm in their list of wavelengths to include 810-830nm and then jumps to 904nm. At this point it is rather laughable that these ranges are specifically excluding 850nm.
This list of quotes above would lead us to question if these researchers even consider 850nm as a viable wavelength at all, not even bothering to debate if 850nm is the best.
What would cause these researchers to forget about 850nm, the supposedly "best" wavelength acclaimed by many brands?
Did these researchers miss the memo about how great 850nm is? Or are they just following the actual evidence?
810nm Vs 830nm - The Real Best Wavelengths:
All of the quotes in the previous section always include 810nm and 830nm wavelengths in their optimal ranges.
So in reality, the debate should be between 810nm and 830nm for the crown of best NIR wavelength, especially now that we know 850nm has been dethroned.
One excellent review article on Photobiomodulation Mechanisms published in 2020 by a long list of 14 researchers had this to say:
"The optimum wavelength in treatment is usually considered to be 810 nm [11]." [9]
In very clear terms, this group of researchers seem to be in agreement that 810nm is typically considered to be the best wavelength.
An interesting 2022 PBM article had this to say:
"The 810nm LED is the most commonly used light sources in the field of PBM" [10]
A 2023 review of wavelengths used for Aspects of Muscle Function (they abbreviate to AoMF) had this to say as a conclusion:
"However, regarding the wavelength of the low power laser, it is hypothesized that wavelengths of 808 – 810nm promote more satisfactory results for AoMF, as approximately 37.5% of favourable studies used this wavelength." [2]
These quotes would lead us to believe that 810nm is not only the optimal wavelength, but has a high number of successful studies to support it.
However, a free article from a 2017 textbook on Photomedicine had this to say about the optimal wavelength:
We finally believe that 830 nm offers very interesting properties compared with other wavelengths, making it the wavelength of choice because of its superior depth of penetration, and larger number of cells and targets it has been shown to photoactivate." [11]
Indeed, we find many articles by Dr. Calderhead and many prominent researchers expressing a favoritism for 830nm. We will explain why in the mechanisms section.
We could not find any peer-reviewed published literature clearly stating that 850nm should be considered the optimum wavelength. If you do find any, please email us a link.
Splitting Hairs - 810nm Vs 830nm
With 810nm and 830nm being very close to each other on the wavelength spectrum with only a 20nm difference between them - it would be very challenging to discern a difference in overall benefits without large-scale trials. So far we have not found any studies directly comparing the effects of both 810nm and 830nm under the same conditions.
In one interview, Dr. Hamblin states that all the low-800's and all the mid-600's have the same benefits. Even the Red and NIR wavelengths have the same benefits. Thus, perhaps making this entire blog a moot point.
One study may have confirmed this observation by showing that an 800nm Laser and 850nm Laser had non-significant differences (i.e. they were the same results).
"Moreover, 800 nm and 850 nm lasers produced identical, non-significant (p > 0.05) PBM effects on the human forearm in vivo in all three (or four) physiological metrics. This observation is expected since the light absorption and scattering properties of blood and CCO are very similar in the wavelength range between 800 and 850 nm. " [10]
You can see the above quote discussing how wavelengths in the 800-850nm range are generally expected to produce the same benefits because they have similar optical properties and absorption mechanisms.
Update: One study compared 800nm vs 850nm laser on transcranial application (through the forehead) on human subjects. They found a much more significant response from 800nm compared to 850nm. [30]
However, in this one case we will temporarily ignore Dr. Hamblin's guidance and continue our analysis.
Penetration Depth - 810nm vs 830nm
The deepest penetration wavelength is often considered to be 810nm. This is the lowest intersection of all of the primary absorbing molecules of the skin (blood, melanin, water). Shorter wavelengths will have less penetration by superficial absorption from melanin and blood. Longer wavelengths will have less penetration by superficial absorption from water.
An article by Dr. Jan Tuner states this concept plainly:
"And, actually, it is the other way around, or, rather with red having low penetration, *810 nm is the best and then penetration is lowered as the wavelength is further increased." [12]
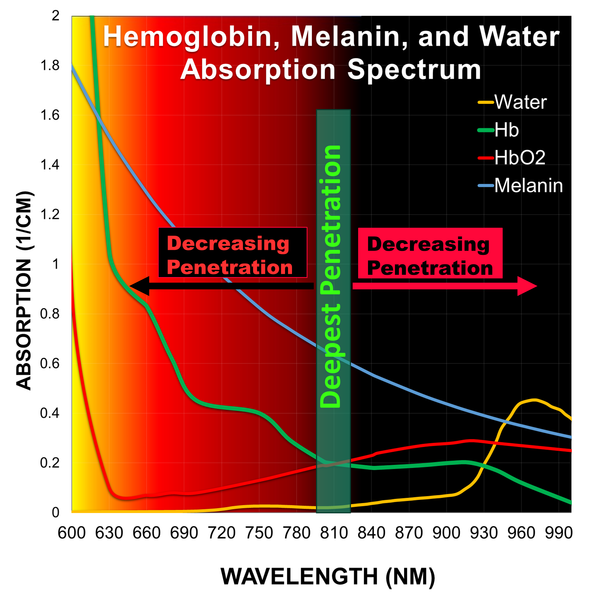
Which would be a detriment to our case for 830nm, as it is implied that 830nm would have slightly less penetration due to more water absorption - and even worse for 850nm. However, this is balanced out by the fact that melanin absorption continues to decrease with longer wavelengths.
Another review article on PBM for a recent viral respiratory illness noted this about the optical windows for best penetration being around 810nm and 1064nm.
"More current investigations have identified distinct optical windows within the near infrared spectrum (810nm and 1064nm) with marked differences in production of oxygenated hemoglobin and cytochrome c oxidase [59]. " [13]
However, once again there are other researchers believing that 830nm has the best penetration.
"Deepest penetration is achieved around 830 nm in the near infrared. " [11]
The above article shows a diagram that measured penetration of wavelengths through a human hand, with clearly the deepest point of penetration was 830nm.
One review article on brain health did observe a similar penetration between 810nm and 830nm through the skull.
"On the other hand, no significant difference has been shown between light penetration through the human skull for LED (830 nm) and laser (810 nm) light [95]." [14]
This is made even more impressive that the 830nm was LED and 810nm was Laser, which typically we assume LED has less penetration than laser due to the divergent beam angle of LED and non-coherence.
Penetration Lost - Skin Contact Vs Non-Contact
We have pointed out in previous blogs that targeting deeper tissue and optimizing penetration requires using the skin contact technique. Many "experts" have wrongfully emphasized the importance of wavelengths, intensity, and pulsing for deep penetration; while conveniently ignoring the skin contact method while selling their affiliated non-contact panels.

We covered in previous blogs that non-contact (at a distance) treatment is inherently superficial penetration regardless of wavelength. Using skin contact not only improves absorption with less reflection losses, but changes the skin optics by providing optical coupling, compressing the skin, and blanching out superficial blood.
As such, even if we concede that 810nm has the best penetration by a small margin - the promise of deep penetration is only delivered with skin-contact devices.
Studies on brain health with 808nm/810nm lasers tend to use skin contact to ensure you are getting the full penetration possible. [14]
The popular clinically-studied Vielight headset devices use 810nm LEDs pressed onto the head and encourage users to part the hair so it can make direct contact to the scalp. [15]
In other words, 810nm is only considered the superior wavelength in the context of achieving deep penetration with skin contact. The aspect that makes 810nm optimal is squandered when used in non-contact LED panels.
When used in non-contact therapy like LED panels, we need to re-evaluate the effectiveness based on more superficial systemic mechanisms. Which opens the door for 830nm to be the most viable candidate especially in LED systems and non-contact delivery.
Mechanisms and Systemic Effects - 830nm
The mechanism department is where 830nm truly shines. The most widely accepted mechanism for red light therapy has been the absorption into Cytochrome C Oxidase (CCO).
In the seminal research by leading researcher Dr. Tiina Karu, she notes the absorption peaks at the following wavelengths:
"with well-pronounced maxima at 620, 680, 760 and 825 nm."
http://photobiology.info/Karu.html
More importantly, each peak corresponds to a specific oxidized or reduced state of the iron (heme) or copper (Cu) molecules in CCO.
For example 760nm corresponds to the reduced state of CuB. So even though 760nm does have an absorption peak, this particular wavelength range in the 700's is often found to be not particularly effective. Perhaps due to this particular Cu state not utilizing the absorbed energy in a beneficial way.
"Low biochemical activity occurs in wavelengths in the range of 700–770 nm." [9]
Light doesn't just need to be simply absorbed by CCO, but it needs a mechanism of action from that absorption. Absorption into the 760nm chromophore is not very effective. So we need to find the absorption peak that corresponds to the best biological response.
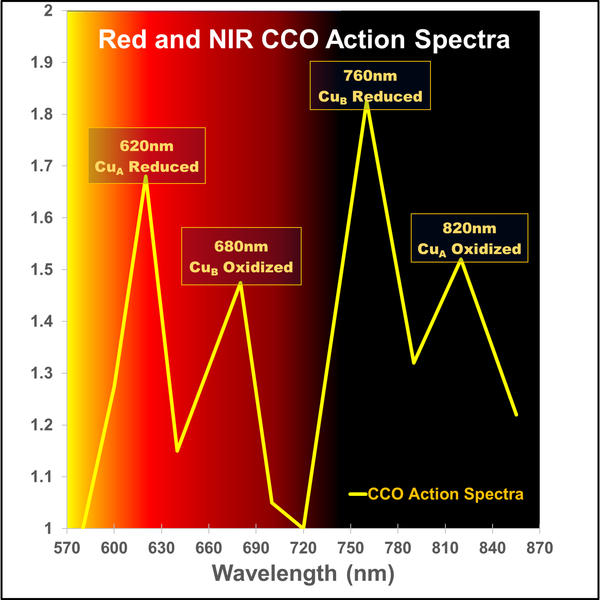
Graph adapted from http://photobiology.info/Karu.html
Another study describes the configuration of the molecules as follows corresponding to their absorption peaks:
"CCO has absorption peaks in the red (Heme a, 605 nm; CuA reduced, 620 nm; heme a3/CuB, 655 nm; CuB oxidized, 680 nm) and the NIR spectral regions (CuB reduced, 760 nm; CuA oxidized, 825 nm) [36,37]. When light is shone on CCO, photon energy is absorbed by the various metal centers of CCO and their electrons are excited from the ground state to upper excited states [38]." [14]
Essentially, researchers have found that targeting the CuA in the Oxidized state leads to tremendous response and benefits - which is at the 825nm peak.
It should go without saying that 830nm is closer to the peak of 825nm than 810nm for the purposes of this debate.
"The oxidized form of cytochrome c oxidase has a broad absorption band above 800 nm that is centered at 830 nm (62)."
http://photobiology.info/Karu.html
In fairness to 810nm and 850nm; the peak for CCO is around 830nm has a "broad absorption band" meaning that by proximity then 810nm and 850nm will also activate the same chromophore to a lesser extent. Confirming why these wavelengths ultimately all have similar benefits.
Now we can see why many subsequent studies have specifically chosen 830nm for it's superior absorption peak in CCO and mechanism of action.
Brain Benefits of 830nm vs 810nm:
The Near Infrared wavelengths are often preferred for deeper tissue treatments like targeting the brain.
Most prominently is that 810nm is the preferred wavelength for transcranial Photobiomodulation (targeting the brain through the head) due to it's promise of having the deepest penetration, as one review article for tPBM had this to say:
"When we investigated the wavelength selection for transcranial LLLT in SCI-indexed articles and other published reports, we found that the most frequently used and concerned wavelength was 810 nm (Fig. 1)." [16]
Another 2023 review article on transcranial photobiomodulation had this to say about a common successful dosing protocol for the brain.
"One of the most common protocols for clinical populations employed devices delivering near-infrared light (810 nm), the irradiance of 20-25 mW/cm2, and fluence of 1-10 J/cm2." [17]
Clearly, 810nm is one of the most-used wavelengths for brain health.
However, 830nm often has it's fair share of studies on the brain. Most notably several studies have used 830nm LED devices on the brain for depression and anxiety disorder in humans. [18][19]
They often state something like this about the choice of wavelength:
"The benefits of t-PBM are wavelength specific: a mitochondrial enzyme, cytochrome c oxidase, is the primary chromophore for the t-PBM with peak absorption close to 830 nm.7" [19]
These quotes confirm a tradeoff that while 810nm promises the best penetration making it preferred for transcranial targets, 830nm is often selected for it's superior mechanisms of targeting the CCO absorption peak. Both of which are very important for brain benefits.
Skincare and Superficial LED Devices with 830nm:
Some actual clinical-grade and clinically studied LED devices have used 830nm in a non-contact delivery system.
These devices are the Healite II and the Omnilux LED system (not the masks, the clinical grade panels they sell). [20]
These have been studied for a range of benefits particularly for wound healing and dermatology. [20]
An important paper titled "Is light-emitting diode phototherapy (LED-LLLT) really effective?" in 2011 lays the groundwork for the scientific backing for the LED panel craze we know today. If it weren't for the success of these early LED panels using 830nm, then LEDs would likely not be considered a viable theraputic option.
"The LED system being used must have first of all, and most importantly, the correct wavelength for the target cells or chromophores. At present, the published literature strongly suggests 830 nm for all aspects of wound healing, pain, anti-inflammatory treatment and skin rejuvenation" [21]
With this quote really establishing that 830nm is preferred for a wide range of benefits from wound healing, pain, inflammation, and even skin rejuvenation - particularly for LED systems. As well it offers the ideal wavelength for the target chromophores and mechanisms regardless of penetration.
This is where the versatility of 830nm NIR shines for superficial wounds and skincare - not only for deep tissue treatments. Where typically NIR is not considered for skincare.
In fact, one study compared a 633nm and 830nm LED panel for skincare and found that the 830nm wavelength gave more satisfactory results than the 633nm. Which debunks the myth that many people falsely prefer Red for skincare. And they found the combination of 633nm and 830nm gave the best overall results for skincare. [22]
Other benefits of 830nm:
An excellent 2016 study covers the use of the Healite 830nm LED panel on treating 395 injuries in student athletes over a 15 month period, with resounding success in most treatments. The discussion section shows much favorability for 830nm LED treatments especially for the systemic response. [23]
One study compared different wavelengths for hair growth in animals, and found that 830nm performed better than 632, 670, and 785nm. [24]
One study on supporting eye health used 830nm on rodent retinas and found very good mitochondrial support and protection. So while there is a lot of hype around 670nm for eye health, it is clear there is some preliminary research that 830nm NIR will be very helpful for the eyes as well. [25]
So we can see many studies identify a possibility unexplored potential for 830nm to support everything from brain health to skincare to hair and eye health. As well the Near-Infrared 830nm is changing some misconceptions that people are incorrectly avoiding NIR for eye health and skin health.
Conclusions:
While 810nm may have the best penetration, the real benefits of red light therapy rely on absorption and activation of specific chromophores and biological mechanisms. This is where 830nm has been shown to be superior.
For targeting deeper tissue, then a skin-contact device with 810nm would be ideal to make sure enough photons reach the target tissue.
For a wider range of versatility from deep tissue to skincare based on peak absorption mechanisms - the optimal choice of wavelength is 830nm. Non-contact devices like commercial LED panels need to focus more on wavelengths with systemic benefits due to the lack of penetration.
As always, we can get too far down a rabbit hole and lose perspective. It may be redundant to debate the benefits of 810nm, 830nm, and 850nm due to their close proximity on the spectrum and similar penetration and mechanisms.
Remember that wavelengths alone do nothing. It is extremely reductive when brands and "experts" make a list of medical claims based on a wavelength alone and then sell devices that are completely different than the studies used. It is the proper implementation of dosing, the device parameters, how it is used, and the bio-individuality of the patient that truly determines the benefits. Understanding context is how we can identify that certain wavelengths are more suitable for skin-contact technique vs non-contact method as a major factor.
Based on this blog's findings - why include 850nm at all in devices? While the Red 600-700nm and NIR 800-840nm focus on CCO absorption mechanisms - longer wavelengths like 840nm+ will start to focus more on the other two important PBM mechanisms of developing EZ water in the cells and modulating light-gated ion channels. So by including 850nm we can access more synergistic mechanisms than if we only used 810 or 830nm. We cover this more in a previous blog.
1064nm was also overlooked as a potential wavelength for red light therapy based on the lack of CCO absorption. So even though 1064nm has great penetration (perhaps better than 810nm), it was thought that 1064nm wouldn't activate any beneficial mechanisms. Until now that the mechanisms of EZ Water and Light Gated Ion channels has been accepted, as well as more studies and devices confirming benefits in clinical trials with 1064nm. [29]
Most of the full-body red light therapy studies have indeed used 660nm+850nm LEDs in the NovoThor pod. Unfortunately in this industry if we say something is not optimal, it is mistaken for us saying it is not effective. 850nm is certainly effective, just not optimal.
So what do you think is the best wavelength? Is this blog biased and cherry picked? If this blog was cherry picked, then someone should be able to easily provide dozens of direct quotes from published literature plainly stating that 850nm is optimal, has ideal penetration, and activates beneficial mechanisms specific to this wavelength - as we have done in this blog for 810nm and 830nm.
References:
[1]
Hamblin MR. Photobiomodulation for traumatic brain injury and stroke. J Neurosci Res. 2018 Apr;96(4):731-743. doi: 10.1002/jnr.24190. Epub 2017 Nov 13. Erratum in: J Neurosci Res. 2019 Mar;97(3):373. PMID: 29131369; PMCID: PMC5803455.
[2]
Cubas IH, Eckert JA, Canalli LV, Carvalho AR D, Bertolini GR F. Photobiomodulation in aspects of muscle function – a scoping review. J Pre Clin Clin Res. 2023;17(1):32-36. doi:10.26444/jpccr/161689.
[3]
Zhang, Chun-Xia et al. “Considerations for the Use of Photobiomodulation in the Treatment of Retinal Diseases.” Biomolecules vol. 12,12 1811. 3 Dec. 2022, doi:10.3390/biom12121811
[4]
Keshri, Gaurav K et al. “Photobiomodulation with Pulsed and Continuous Wave Near-Infrared Laser (810 nm, Al-Ga-As) Augments Dermal Wound Healing in Immunosuppressed Rats.” PloS one vol. 11,11 e0166705. 18 Nov. 2016, doi:10.1371/journal.pone.0166705
[5]
Askalsky, Paula, and Dan V Iosifescu. “Transcranial Photobiomodulation For The Management Of Depression: Current Perspectives.” Neuropsychiatric disease and treatment vol. 15 3255-3272. 22 Nov. 2019, doi:10.2147/NDT.S188906
[6]
Bath, A.S., Gupta, V. Cardio-light: nitric oxide uncaged. Lasers Med Sci 34, 405–409 (2019). https://doi.org/10.1007/s10103-018-2671-x
[7]
Taylor, David N et al. “Low-Level Laser Light Therapy Dosage Variables vs Treatment Efficacy of Neuromusculoskeletal Conditions: A Scoping Review.” Journal of chiropractic medicine vol. 19,2 (2020): 119-127. doi:10.1016/j.jcm.2020.06.002
[8]
Pires de Sousa, Marcelo Victor et al. “Transcranial low-level laser therapy (810 nm) temporarily inhibits peripheral nociception: photoneuromodulation of glutamate receptors, prostatic acid phophatase, and adenosine triphosphate.” Neurophotonics vol. 3,1 (2016): 015003. doi:10.1117/1.NPh.3.1.015003
[9]
Dompe, Claudia et al. “Photobiomodulation-Underlying Mechanism and Clinical Applications.” Journal of clinical medicine vol. 9,6 1724. 3 Jun. 2020, doi:10.3390/jcm9061724
[10]
Pruitt, T.; Carter, C.; Wang, X.; Wu, A.; Liu, H. Photobiomodulation at Different Wavelengths Boosts Mitochondrial Redox Metabolism and Hemoglobin Oxygenation: Lasers vs. Light-Emitting Diodes In Vivo. Metabolites 2022, 12, 103. https://doi.org/10.3390/metabo12020103
[11]
Calderhead, Robert Glen, and Yohei Tanaka. ‘Photobiological Basics and Clinical Indications of Phototherapy for Skin Rejuvenation’. Photomedicine - Advances in Clinical Practice, InTech, 17 May 2017. Crossref, doi:10.5772/intechopen.68723.
[12]
Tunér J. The Laser Wound Healing Contradiction. Photomed Laser Surg. 2015 Jun;33(6):343-4. doi: 10.1089/pho.2015.3905. PMID: 26067944.
[13]
Kitchen, Lydia C et al. “Rationale for 1068 nm Photobiomodulation Therapy (PBMT) as a Novel, Non-Invasive Treatment for COVID-19 and Other Coronaviruses: Roles of NO and Hsp70.” International journal of molecular sciences vol. 23,9 5221. 7 May. 2022, doi:10.3390/ijms23095221
[14]
Salehpour, Farzad et al. “Brain Photobiomodulation Therapy: a Narrative Review.” Molecular neurobiology vol. 55,8 (2018): 6601-6636. doi:10.1007/s12035-017-0852-4
[15]
Zomorrodi, Reza et al. “Pulsed Near Infrared Transcranial and Intranasal Photobiomodulation Significantly Modulates Neural Oscillations: a pilot exploratory study.” Scientific reports vol. 9,1 6309. 19 Apr. 2019, doi:10.1038/s41598-019-42693-x
[16]
Wang P, Li T. Which wavelength is optimal for transcranial low-level laser stimulation? J Biophotonics. 2019 Feb;12(2):e201800173. doi: 10.1002/jbio.201800173. Epub 2018 Oct 1. PMID: 30043500.
[17]
Lee TL, Ding Z, Chan AS. Can transcranial photobiomodulation improve cognitive function? A systematic review of human studies. Ageing Res Rev. 2023 Jan;83:101786. doi: 10.1016/j.arr.2022.101786. Epub 2022 Nov 9. PMID: 36371017.
[18]
Cassano, Paolo et al. “Transcranial Photobiomodulation for the Treatment of Major Depressive Disorder. The ELATED-2 Pilot Trial.” Photomedicine and laser surgery vol. 36,12 (2018): 634-646. doi:10.1089/pho.2018.4490
[19]
Maiello, Marco et al. “Transcranial Photobiomodulation with Near-Infrared Light for Generalized Anxiety Disorder: A Pilot Study.” Photobiomodulation, photomedicine, and laser surgery vol. 37,10 (2019): 644-650. doi:10.1089/photob.2019.4677
[20]
Ablon, Glynis. “Phototherapy with Light Emitting Diodes: Treating a Broad Range of Medical and Aesthetic Conditions in Dermatology.” The Journal of clinical and aesthetic dermatology vol. 11,2 (2018): 21-27.
[21]
Kim, Won-Serk, and R Glen Calderhead. “Is light-emitting diode phototherapy (LED-LLLT) really effective?.” Laser therapy vol. 20,3 (2011): 205-15. doi:10.5978/islsm.20.205
[22]
Lee SY, Park KH, Choi JW, Kwon JK, Lee DR, Shin MS, Lee JS, You CE, Park MY. A prospective, randomized, placebo-controlled, double-blinded, and split-face clinical study on LED phototherapy for skin rejuvenation: clinical, profilometric, histologic, ultrastructural, and biochemical evaluations and comparison of three different treatment settings. J Photochem Photobiol B. 2007 Jul 27;88(1):51-67. doi: 10.1016/j.jphotobiol.2007.04.008. Epub 2007 May 1. PMID: 17566756.
[23]
Foley, John et al. “830 nm light-emitting diode (led) phototherapy significantly reduced return-to-play in injured university athletes: a pilot study.” Laser therapy vol. 25,1 (2016): 35-42. doi:10.5978/islsm.16-OR-03
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4846838/
[24]
Kim TH, Kim NJ, Youn JI. Evaluation of wavelength-dependent hair growth effects on low-level laser therapy: an experimental animal study. Lasers Med Sci. 2015 Aug;30(6):1703-9. doi: 10.1007/s10103-015-1775-9. Epub 2015 Jun 6. PMID: 26048721.
[25]
Gopalakrishnan, S., Mehrvar, S., Maleki, S. et al. Photobiomodulation preserves mitochondrial redox state and is retinoprotective in a rodent model of retinitis pigmentosa. Sci Rep 10, 20382 (2020). https://doi.org/10.1038/s41598-020-77290-w
[26]
Water Absorption Coefficient Spectrum:
https://omlc.org/spectra/water/data/hale73.txt
https://omlc.org/spectra/water/abs/
[27] Hemoglobin Absorption Coefficient Spectrum:
https://omlc.org/news/jan98/skinoptics.html
https://omlc.org/spectra/hemoglobin/summary.html
[28] Melanin Absorption Coefficient Spectrum:
https://omlc.org/spectra/melanin/mua.html
[29]
Kitchen, Lydia C et al. “Rationale for 1068 nm Photobiomodulation Therapy (PBMT) as a Novel, Non-Invasive Treatment for COVID-19 and Other Coronaviruses: Roles of NO and Hsp70.” International journal of molecular sciences vol. 23,9 5221. 7 May. 2022, doi:10.3390/ijms23095221
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9105035/
[30]